Introduction
Chronic heel pain is a common foot ailment. This pain can be due to degeneration of the connective tissue that supports the heel (plantar fasciitis), stress fractures on the heel’s bone (calcaneus) or nerve entrapment (Baxter’s). Baxter’s nerve entrapment (a type of peripheral neuropathy) accounts for approximately 20% of chronic heal cases,1 however, it is often misdiagnosed due to its symptomatic similarities to plantar fasciitis.
What is Baxter’s Nerve?
The Baxter’s nerve (also known as the inferior calcaneal nerve) is the first branch of the lateral plantar nerves that enter through the tarsal tunnel to innervate the feet. The lateral plantar nerves are responsible for enabling sensation to the skin, heel bone (calcaneal periosteum), ligaments (long plantar ligament) and muscles of the foot (digiti minimi, flexor digitorum brevis and quadratus plantae).2 However, Baxter’s nerve itself enables sensation in the muscles of the inner ankle and arches of the feet. It can also act as a motor nerve to move the abductor digiti minimi (fifth toe) muscle.
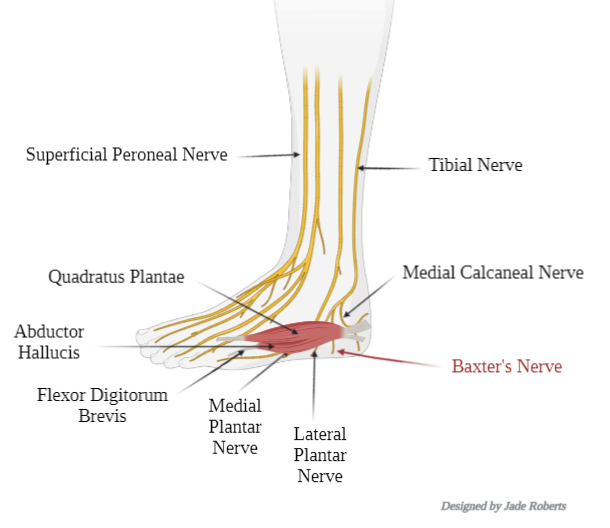
As illustrated in the figure above, the nerve lies vertically between the abductor hallucis and quadratus plantae muscles, it then makes a sharp 90° horizontal turn to lie under the heel bone (calcaneal periosteum) to innervate the abductor digiti minimi (fifth toe) muscle.
Causes
The exact cause of Baxter’s nerve entrapment is unknown. However, its location, as illustrated in the figure below (sourced from Toye, 2012),3 can make it prone to nerve compression for two reasons:
- The nerve turns laterally to be in between the abductor hallucis (AH) (muscle on the inner side of the ankle) and the quadratus plantae (QP) (muscle that runs from the inner ankle to the top of the foot).2
- This nerve also turns sharply into the front of the heel bone and the inner arch of the foot. This area has a lot of contact on the floor and resulting pressure on the foot.2
Risk Factors
Certain conditions make an individual more susceptible to Baxter’s nerve entrapment,4 these include:
- Over-pronation (flatness) of the feet
- Calcaneal spur (bony outgrowth from the heel of the foot)
- Calcaneal (heel bone) stress
- Plantar fasciitis
- Vascular (blood vessels) enlargement in the foot
- Muscular enlargement in the foot (exemplified in athletes)
- Ageing
Symptoms
The symptoms of Baxter’s nerve entrapment include:
- Sharp or burning sensation around the inner area of the heel
- Pins and needles around the inner area or the sole of the heel
- Pain around the inner area or the sole of the heel
- Pain when pressure is applied (e.g. walking or running) around the inner area or the sole of the heel
Other conditions that can present like Baxter's nerve entrapment
Baxter’s nerve entrapment is often misdiagnosed for its symptomatic similarities to other chronic heel pain ailments.
Heel Bursitis: Bursae are small fluid-filled sacs in the heel near the Achilles tendon. They can either be retrocalcaneal (found between the Achilles tendon and heel bone) or subcutaneous calcaneal (found between the skin at your heel and achilles tendon). These sacs cushion the heel and tendon to prevent friction when they rub against each other. Bursitis occurs when the bursa becomes irritated due to high-stress factors such as running or inappropriate shoes (e.g. high heels or tight fitting shoes).
Morton’s Neuroma: Occurs when a nerve between the bones of the forefoot becomes irritated or damaged. As a result the surrounding tissue becomes thickened and inflamed. Intermetatarsal bursitis (bursa that is adjacent to the neuroma) can occur simultaneously with Morton’s neuroma. Morton’s neuroma tends to be more prevalent in women and is often due to the prolonged use of high heels. However, it can also occur with tight fitting shoes or ageing.
Midfoot Osteoarthritis: Midfoot osteoarthritis is a progressive, degenerative condition that causes the joints in the middle of the foot to become painful and stiff. The bones that are classified as midfoot include: the cuboid, the navicular, the lateral, middle and medial cuneiform. There are many acquired (e.g. joint injury) or genetic (age, sex, familial history and obesity) factors that can contribute to midfoot arthritis.
Plantar Fasciitis: The plantar fascia is a thick ligament that connects the big toe to the heel bone. Much like a spring, it has a recoil mechanism that pushes you forward when you walk or run. The ligament is under enormous pressure (especially during running), and as a result can become irritated and painful.
- Differentiating between Baxter’s nerve entrapment and plantar fasciitis: The symptoms between plantar fasciitis and Baxter’s nerve entrapment are very similar, however, there are some distinct symptoms between the two.5 Baxter’s nerve entrapment tends to have:
- A less occurrence of morning pain in the feet. In contrast, with plantar fasciitis, the pain tends to increase as the day goes on.
- Sensations such as numbness, tingling, and pins and needles in the feet. Whereas, plantar fasciitis does not.
- The inside of the heel hurts directly when touched, unlike plantar fasciitis.
Diagnosis
Diagnosis for Baxter’s nerve entrapment is often differential and multifaceted due to its symptomatic overlap with other chronic heel pain. It comprises of three different phases:
- Clinical interview
- Clinical testing
- Diagnostic ultrasound
Clinical Interview
This phase involves your GP conducting an interview about your full medical history.6 Some common questions that are asked include:
- Have you had any previous injuries?
- How did your pain start?
- Have you had any previous treatments for your pain?
- What treatments have you found helpful and unhelpful?
- Do you suffer from other diseases? (This is to rule out other medical conditions that may contribute to your pain.)
Clinical Testing
After the interview, your GP will ask you to perform physical tasks.6 They will also perform a Windlass diagnostic test, which involves stretching the foot backwards (dorsiflexion) and feeling the area with slight pressure. Any pain associated with certain tasks can be indicative of the reason for chronic heel pain. They may also feel your ankle, foot and leg, particularly in the area of the nerve. The signs they look out for are:
- Restricted bending or contraction of your foot (dorsiflexion)
- A limp or a preference to tip toeing
- Pain when walking barefoot on hard surfaces or climbing up the stairs
- A sudden increase in physical activity involving your feet prior to the onset of the symptoms
Diagnostic Ultrasound
Ultrasound can be an effective tool in diagnosing Baxter’s nerve entrapment due to it being cheap, accessible and rapid. It further allows the flexibility to move the imaging probe around various areas of the ankle and foot. During an ultrasound, differential diagnosis occurs and the physician can rule out:
- Plantar Fasciitis: By checking for the thickness and tears in the plantar fascia ligament which runs longitudinally across the foot.7
- Medial Calcaneal Nerve Entrapment: This can also cause pain in the tarsal tunnel muscles of the foot (i.e. posterior tibialis, flexor digitorum longus, and flexor hallucis longus) causing a similar pain to Baxter’s nerve entrapment.7
- Tibial Nerve Issues: Any lesions or engorgements in the tibial nerve can be ruled out for chronic heel pain.7
- Tears Of The Tibial Tendon: Tears in the posterior tibial tendon can cause the heel arch to collapse, further resulting in heel pain.7
- Other Factors: Coalition (joining of two bones), stress fractures or bone cysts.7
If the ultrasound does not provide a defined result, computerised tomography (CT) or magnetic resonance imaging (MRI) can be used for diagnosis.
Treatments
Treatments can often start with simple measures to control the pain using physiotherapy. However, Baxter’s nerve entrapment is not easy to treat and often needs more invasive measures such as ultrasound-guided injections and surgery.
Physiotherapy
Physiotherapy to manage the pain is a combination of a rehabilitation programme alongside manual therapy techniques (a more hands-on approach).6
The rehabilitation programme includes:
- Pain Management Advice: Use of cold or heat therapy, and the use of oral or topical NSAIDs (pain medication).
- Personalised Exercise Plan: Inclusive of strengthening exercises and stretching to alleviate pain.
- Advice On Returning To Exercise: Incorporating appropriate rest periods as per the level of pain.
Manual therapy includes:
- Transcutaneous Electric Nerve Stimulation: A process where electric currents are delivered to the affected area in order to relieve pain.
- Acupuncture: A process where needles are inserted into the affected area to relieve pain and promote recovery.
- Massage Therapy
- Taping
- Orthotics: Shoe inserts or night splints to relieve pain.
Ultrasound Guided Injections
Due to the size and depth of Baxter’s nerve, along with the numerous arteries and veins surrounding it, ultrasound is used to guide an injection with the medication to the right place. Steroids (anti-inflammatory medication) and local anaesthesia (numbing agent) are injected near the nerve. Ultrasound guided steroid injections are shown to be very effective in treating Baxter’s nerve entrapment as it provides long-lasting pain relief.8 However, the steroid injections should be used in conjunction with physiotherapy.
Surgery
When ultrasound sound guided injections fail to target pain effectively, surgery is the last resort of treatment. Neurolysis is a form of surgery which destroys the nerve and ceases pain by interrupting the signals responsible for transmitting pain. There are a number of ways to destroy the nerve: injection of alcohol directly into the nerve or ablation with heat.
Summary
Baxter’s nerve entrapment is a tricky disease to navigate around due to its difficult diagnosis, other diseases of chronic heel pain often mask it. However, it is important to remember that Baxter’s nerve entrapment is manageable, as long as appropriate measures (such as physiotherapy, exercise and appropriate footwear) are done alongside invasive treatments.
References
- Öztuna V, Ozge A, Eskandari MM, Çolak M, Gölpinar A and Kuyurtar F. Nerve Entrapment in Painful Heel Syndrome’. Foot & Ankle International, 2002;23(3):208–11. Available from: doi.org/10.1177/107110070202300304>
- DJ Arenson, GL Cosentino, and SM Suran. The Inferior Calcaneal Nerve: An Anatomical Study. Journal of the American Podiatric Medical Association.1980;70(11):552–60. Available from: <doi.org/10.7547/87507315-70-11-552>
- Toye LR. Baxter’s Nerve (First Branch of the Lateral Plantar Nerve) Impingement. [online]. Radsource: US; 2012. Available from: https://radsource.us/baxters-nerve/
- OnePointHealth. What Is Baxter’s Nerve Entrapment. [date unknown] [Accessed 15 May 2022] Available from: https://onepointhealth.com.au/conditions/baxters-nerve-entrapment/.Masci L. Chronic Heel Pain: Is It Baxter’s Nerve Entrapment?. Sport Doctor London.2021. Available from: https://sportdoctorlondon.com/baxters-nerve-entrapment/
- Ultrasound Guided Injections. ‘Baxter’s Nerve Entrapment’.2020. Available from: https://www.ultrasound-guided-injections.co.uk/baxters-nerve-entrapment/
- Baravarian B, ‘A Closer Look At Imaging Options for Complicated Heel Pain’. Foot and Ankle Blog, 2018. Available from: https://www.footankleinstitute.com/blog/closer-look-at-imaging-for-heel-pain/
- Presley JC, Maida E, Pawlina W, Murthy N, Ryssman DB, Smith J Sonographic Visualization of the First Branch of the Lateral Plantar Nerve (Baxter Nerve): Technique and Validation Using Perineural Injections in a Cadaveric Model. Journal of Ultrasound in Medicine. 2013;329):1643–52. Available from: <doi.org/10.7863/ultra.32.9.1643>




