


Overview: what is IBS?
Irritable Bowel Syndrome (IBS) is a common yet poorly understood gastrointestinal condition characterised by abdominal pain, altered bowel habits and bloating. It is estimated to affect between 5% and 10% of the population.1
Generally, there is little diagnostic testing for IBS that is used universally, so diagnosis primarily relies on the recognition of multiple symptoms reported by patients, using tools such as the Rome IV criteria and the Bristol stool scale for diagnostic evaluation.
There are four different IBS subtypes according to their stool pattern:
- Diarrhoea predominant IBS (IBS-D)
- Constipation-predominant IBS (IBS-C)
- Mixed-diarrhoea-and-constipation IBS (IBS-M)
- Unclassified IBS
The exact cause of IBS is not known. It is largely understood that when the condition is present, there is disordered communication between the gut and the brain. It is thought that this may result in observed changes to how food is digested and moved throughout the intestinal system, resulting in symptoms like diarrhoea, cramping, and abdominal pain.
As many patients report certain foods inducing their symptoms, various research surrounds the role of food as both a cause for IBS symptoms and as a potential avenue for treatment.2 Research has been focussed on the effect of three main dietary approaches: the traditional dietary advice, the low FODMAP diet, and the gluten-free diet. It remains unclear which of these is the most effective at treating the condition and why.2 The usefulness of medication and probiotics continues to be explored, but with limited information
The role of diet in managing IBS
When it comes to managing IBS through dietary approaches, the traditional dietary advice (TDA) and low FODMAP diet (LFD) are the first and second-line treatments, respectively, in the UK. The gluten-free diet is not officially recommended by healthcare professionals for IBS due to a lack of evidence.3
Traditional dietary advice (TDA)
TDA is comprised of a set of sensible dietary and lifestyle recommendations provided by a medical professional, bolstered with individualised recommendations to manage IBS symptoms. Dietary modifications often include:
- Reducing alcohol intake
- Reducing caffeine intake
- Avoiding spicy food
- Cutting back on dietary fat
- Increasing fluid intake
- Adjusting fibre intake
TDA is a logical first step for treating IBS as it involves adopting a healthy diet and lifestyle, both of which may alleviate or even prevent IBS symptoms in the first place.3 There is evidence supporting the effectiveness of TDA in alleviating IBS symptoms in some patients from Randomised Controlled Trials (RCTs).1
Increased intake of dietary fibre is one of the TDA recommendations, and RCTs have specifically highlighted its benefits in managing IBS symptoms. This may be due to fibres’ role in affecting the stimulation of bowel movements, gut bacteria, the immune system and the hormones and neurotransmitters that help regulate the gut.4
Furthermore, increased alcohol use has been linked with the risk of developing IBS5 and worsening of symptoms once it is present.6 Similar results have been found for caffeine, especially when subjects were also overweight.7 However, the exact role of these substances in IBS remains unclear.
The FODMAPS diet
FODMAP stands for Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols.8 These are short-chain carbohydrates, which include starches, sugars, and fibres found in food. Our body’s enzymes can’t break these down, so instead, we rely on our gut bacteria to ferment them. This fermentation leads to the release of gases, such as carbon dioxide, methane and hydrogen.9 This additional gas, combined with the extra fluid that FODMAPS draw into the gut, can slow digestion down and in susceptible individuals, may result in IBS symptoms.10
This table shows examples of foods that are high-FODMAP and low-FODMAP:
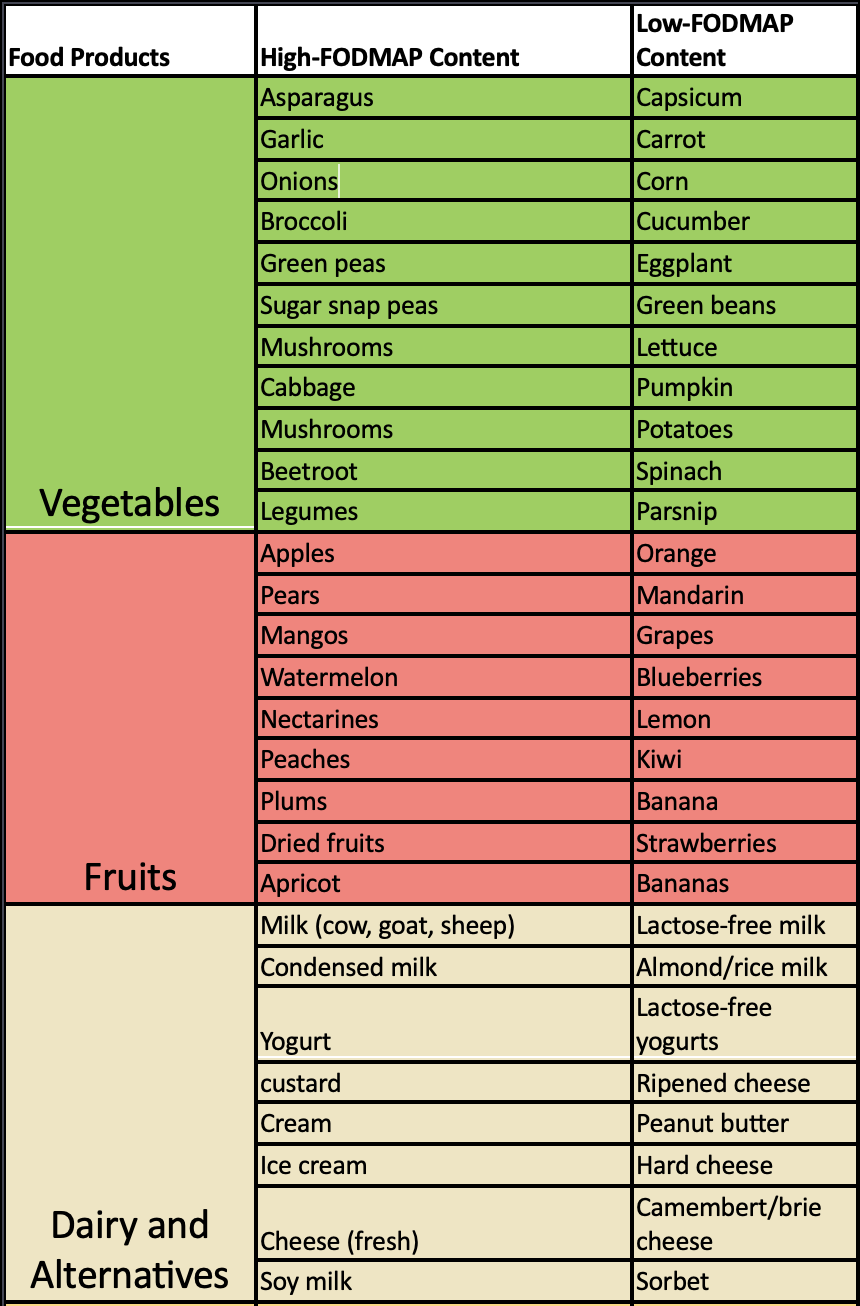
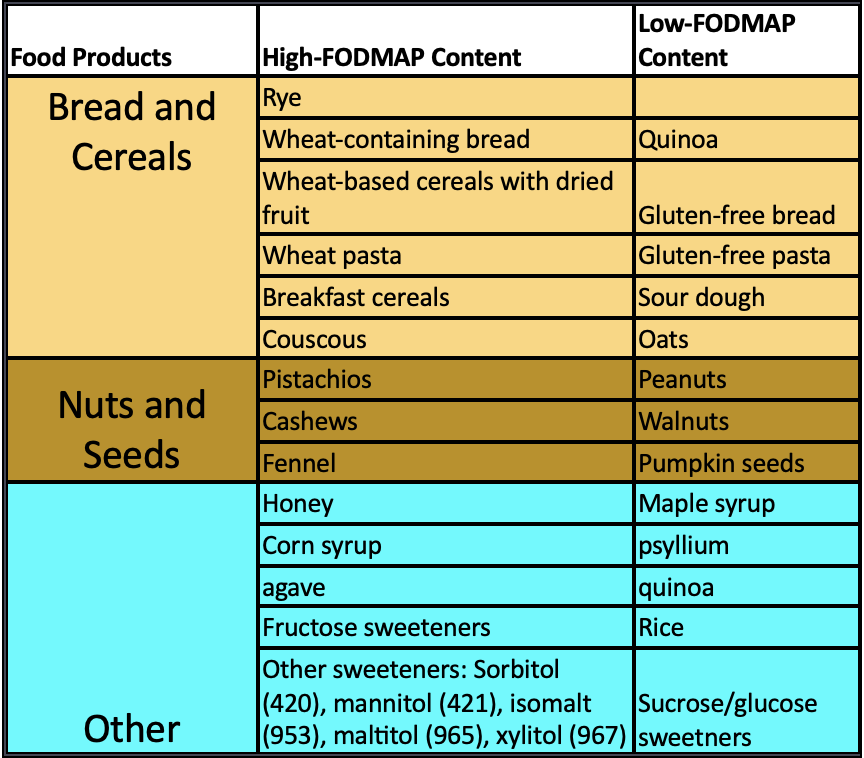
Note these are not exhaustive lists, and there may be other foods within each subcategory.
An individual may only be sensitive to one of these FODMAP foods, so instead of cutting out all these foods from their diet, specific triggers are identified first, prior to removal. This occurs in three key phases:
Elimination Phase. Eliminate all high-FODMAP foods for several weeks. It is essential to work with a nutritionist during this phase as it can be challenging to eliminate all high FODMAP carbohydrates whilst still meeting your nutritional needs. Symptom improvement may occur immediately or over several weeks.
Reintroduction Phase. Systematically reintroduce FODMAPs one at a time to determine which foods can be tolerated and in what quantity. This phase typically spans six to ten weeks.
Personalisation Phase. Modify diet to increase variety whilst adjusting the type and amount of FODMAP carbohydrates based on what was learned during the reintroduction phase.
The low FODMAP diet is not intended to be a long-term solution but rather a temporary approach to manage symptoms whilst identifying specific FODMAP triggers. By adhering to this diet, individuals can identify which FODMAPs they are intolerant to and then customise their dietary choices accordingly whilst maintaining a nutritionally balanced diet.
Both healthy individuals and those with IBS exhibit similar physiological responses to FODMAP ingestion, as demonstrated by MRI imaging. However, individuals with IBS often experience heightened symptoms, marked by hypersensitivity in the abdominal region.11
RCTs have shown that low FODMAP is effective and safe for treating IBS symptoms.12 This may occur due to a reduction of fermentation-produced hydrogen gas and an alteration in the gut bacteria population, such as those that consume hydrogen. The LFD also appears to activate a cluster of nerves known as the Meisner plexus, which helps accelerate digestion.13
Furthermore, some evidence shows the LFD diet may be more effective than other diets, such as the TDA.1 However, there is limited long-term evidence supporting the efficacy of a low FODMAP diet. Studies conducted over 9 months have shown that symptom improvement can be sustained, with 82% of patients on a low FODMAP diet experiencing consistent symptom relief at 9 months, compared to 49% with traditional dietary advice.14
Considerations when using a diet for IBS
Compared to the LFD, the TDA is generally cheaper, less time-consuming to shop for and easier to follow when eating out.1 The LFD also requires consultations with a nutritionist for correct implementation, and it may be difficult to obtain an appointment with someone. There is also limited information on the long-term effectiveness of the LFD.1
Moreover, even when an optimal diet is selected, adopting a holistic approach to dietary and lifestyle changes is crucial. This includes not only adjusting what you eat but also making modifications to other aspects of your daily routine, such as regular exercise and sleep.
Other triggers
Traditional dietary advice extends beyond the realm of FODMAPs and considers other potential triggers for IBS symptoms, such as alcohol and caffeine. When considering the LFD, it is important to consider these other potential triggers mentioned in TDA.
Fibre type
The TDA recommends fibre for managing IBS. Whilst fibre can be beneficial for IBS, it's important to focus on soluble fibre sources like ispaghula, as they tend to be more effective in symptom management compared to insoluble fibre sources like wheat bran. Furthermore, the type of soluble fibre also matters. Short-chain highly fermentable fibres, such as oligosaccharides, can actually worsen symptoms of IBS, whereas long-chain moderately fermentable fibres, such as psyllium, have effects that may improve symptoms.4 A nutritionist will be able to guide you about the correct consumption of fibre sources.
Summary
Whilst the exact cause of IBS remains uncertain, it's believed to involve disordered communication between the gut and the brain. Given that many individuals report specific foods as a trigger for their symptoms, various dietary approaches have been explored.
The two main dietary approaches for managing IBS include traditional dietary advice (TDA) and the low FODMAP diet (LFD). TDA encompasses lifestyle changes such as reducing alcohol and caffeine intake, avoiding spicy foods, and adjusting fibre intake. It is a logical first step, focusing on promoting a healthy diet and lifestyle, with some evidence supporting its effectiveness in providing symptomatic relief. On the other hand, the LFD restricts fermentable carbohydrates (FODMAPs), which can contribute to IBS symptoms. The LFD, although more restrictive, has shown promise in clinical trials and may be more effective than the TDA at reducing symptoms and improving the overall quality of life for many individuals living with IBS, although the long-term effects of the LFD remain unknown.
Choosing the right dietary approach can be challenging, even with professional help, as the most effective recommendations are unclear. Regular consultation with a healthcare professional is fundamental, especially when adopting the LFD and attempting to increase intake of the correct type of fibre. This professional guidance will help establish safe and effective dietary modifications tailored to your individual needs. Additionally, making sure to adopt a holistic approach for IBS management is essential, ensuring that other potential triggers like alcohol, caffeine and sleep are considered.
References
- Rej, Anupam et al. (2022) ‘Efficacy and acceptability of dietary therapies in non-constipated irritable bowel syndrome: A randomized trial of traditional dietary advice, the low fodmap diet, and the gluten-free diet’, Clinical Gastroenterology and Hepatology, 20(12). doi:10.1016/j.cgh.2022.02.045.
- Böhn, L. et al. (2013) ‘Self-reported food-related gastrointestinal symptoms in IBS are common and associated with more severe symptoms and reduced quality of life’, American Journal of Gastroenterology, 108(5), pp. 634–641. doi:10.1038/ajg.2013.105.
- Hajishafiee, M. et al. (2020b) ‘Healthy lifestyle score and Irritable bowel syndrome: A cross‐sectional study in adults’, Neurogastroenterology & Motility, 32(5). doi:10.1111/nmo.13793.
- El-Salhy, M. et al. (2017) ‘Dietary fibre in irritable bowel syndrome (review)’, International Journal of Molecular Medicine, 40(3), pp. 607–613. doi:10.3892/ijmm.2017.3072.
- Hsu, T.-Y. et al. (2015) ‘Alcohol use disorder increases the risk of irritable bowel disease’, Medicine, 94(51). doi:10.1097/md.0000000000002334.
- Reding, K.W. et al. (2013) ‘Relationship between patterns of alcohol consumption and gastrointestinal symptoms among patients with irritable bowel syndrome’, American Journal of Gastroenterology, 108(2), pp. 270–276. doi:10.1038/ajg.2012.414.
- Koochakpoor, G. et al. (2021) ‘Association of Coffee and caffeine intake with irritable bowel syndrome in adults’, Frontiers in Nutrition, 8. doi:10.3389/fnut.2021.632469.
- Gastroenterology Consultants of San Antonio (2023) Low Fodmap Diet for irritable bowel syndrome: IBS treatment, Gastroenterology Consultants of San Antonio. Available at: https://www.gastroconsa.com/patient-education/irritable-bowel-syndrome/low-fodmap-diet/ (Accessed: 21 September 2023).
- Murray, K. et al. (2014) ‘Differential effects of FODMAPs (fermentable oligo-, di-, Mono-saccharides and polyols) on small and large intestinal contents in healthy subjects shown by MRI’, American Journal of Gastroenterology, 109(1), pp. 110–119. doi:10.1038/ajg.2013.386.
- Morariu, I.-D. et al. (2023) ‘Effects of a low-FODMAP diet on irritable bowel syndrome in both children and adults—a narrative review’, Nutrients, 15(10), p. 2295. doi:10.3390/nu15102295.
- Major, G. et al. (2017) ‘Colon hypersensitivity to distension, rather than excessive gas production, produces carbohydrate-related symptoms in individuals with irritable bowel syndrome’, Gastroenterology, 152(1). doi:10.1053/j.gastro.2016.09.062.
- Schumann, D. et al. (2018) ‘Low fermentable, oligo-, di-, Mono-saccharides and polyol diet in the treatment of Irritable Bowel Syndrome: A systematic review and meta-analysis’, Nutrition, 45, pp. 24–31. doi:10.1016/j.nut.2017.07.004.
- Bellini, M. et al. (2020) ‘Low Fodmap Diet: Evidence, doubts, and hopes’, Nutrients, 12(1), p. 148. doi:10.3390/nu12010148.
- Staudacher, H.M. et al. (2011) ‘Comparison of symptom response following advice for a diet low in fermentable carbohydrates (FODMAPs) versus standard dietary advice in patients with irritable bowel syndrome’, Journal of Human Nutrition and Dietetics, 24(5), pp. 487–495. doi:10.1111/j.1365-277x.2011.01162.x.




