 Medical contributor:
Medical contributor: First revision:
First revision: Introduction
Cholangiocarcinoma (pronounced ko-lan-gee-o-car-sin-oh-ma), is a rare type of cancer affecting approximately 1 to 9 people in every 100,000 people. It develops in the bile ducts of the gallbladder, which is why it is also referred to as: ‘Bile Duct Cancer’.
Two questions you may have:
- What are bile ducts?
- What do bile ducts do?
Bile ducts are a series of tubes that make up part of a larger system known as the biliary system,1 which includes the:
- Liver
- Gallbladder
- Bile ducts
Bile ducts connect the gallbladder to the liver and the bowel (specifically the small intestine) and store a substance called bile, which is made in the liver.2 The role of bile once it travels from the liver through the bile ducts to the gallbladder and then to the small intestine is to break down fats from the food we eat.2
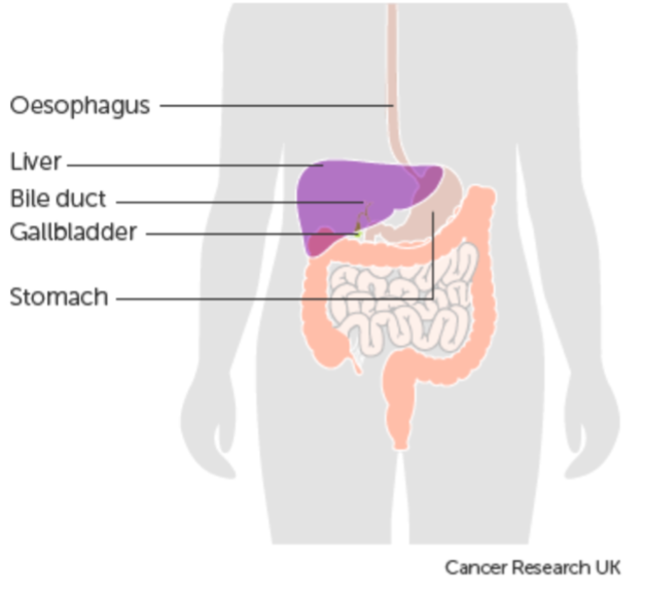
Figure 1: the organ of the biliary system. Image sourced from Cancer Research UK
When tumours form in the bile ducts, the cancerous cells start dividing and growing into the healthy tissues around them. Because bile ducts connect different digestive organs (liver and small intestine), cancer that starts in the bile ducts can spread to nearby connecting organs.
What are the types of cholangiocarcinoma?
Cholangiocarcinoma is a biliary cancer because it affects a part of the biliary system (bile ducts). Remember that bile ducts connect different parts of the biliary system, which means there isn’t just one biliary cancer. In fact, there are 3 main biliary cancers, which are divided based on exactly where they occur in the biliary system.
Intrahepatic bile duct cancer
This type of bile duct cancer develops in the liver itself, as per the name, with hepatocytes being the cells that make up the liver (hence intra (within) and hepatic (liver).
Perihilar / klatskin (extrahepatic) bile duct cancer
This type occurs just outside of the liver where two bile ducts meet (left and right hepatic ducts), to form the common hepatic duct.
Distal (extrahepatic) bile duct cancer
This type of bile duct cancer develops furthest away from the liver, in the bile ducts that are nearer to the small intestine, known as the common bile duct.
What are the risk factors for developing cholangiocarcinoma?
Primary sclerosing cholangitis (PSC) – This is a rare and progressive disease that causes inflammation and scarring to the bile ducts, blocking them from transporting bile from the liver to the small intestine. The exact cause of PSC is not well understood; however, it has been suggested that it is an autoimmune condition whereby the body’s immune system mistakenly attacks healthy tissue- in this case, the bile ducts.3,4
Liver fluke infections – infections caused by a parasite found in raw or undercooked fish have been associated with bile Cholangiocarcinoma. It is believed that the parasite clings to the bile duct wall, which causes inflammation, ulcers, and blockage in the bile ducts, and because the body’s immune system is then thought to mount an inflammatory response, the damage escalates.5,6,7
Other risk factors of cholangiocarcinoma include:
- Other infections, including hepatitis B & C.6,7
- Inflammatory bowel disease (IBD).3
- Bile duct cysts and stones.6
- Chronic liver disease (cirrhosis).7
How does cholangiocarcinoma develop in the body?
Regardless of the risk factors a person may have, it has been suggested that the main ways in which cholangiocarcinoma develops are inflammation and reduced flow of bile through the bile ducts.4
Inflammation
Continued and prolonged inflammation in the bile ducts may cause progressive mutations in genes that prevent cancer cells from forming. This means that cancer cells may then be able to grow and multiply in the damaged bile ducts.4
Reduced flow of bile through the bile ducts
Blocked or damaged bile ducts stop bile from being able to pass from the liver to the small intestine, causing bile to accumulate. When bile accumulates in the bile ducts, the level of acidity in the bile ducts is thought to rise, which can reduce apoptosis (the body’s way of removing damaged cells). If apoptosis is reduced, cells can grow out of control, and tumours can develop from these rapidly growing cells.4
What are the symptoms of cholangiocarcinoma?
The most reported symptoms include:
- Jaundice
- Dark urine
- Stools that resemble greyish clay
- Itching in the skin
- Fever
- Weight loss that is unintentional
- Feeling sick and vomiting
- Feeling tired
- Pain in the stomach
How is cholangiocarcinoma diagnosed?
Physical exam
A doctor should ask a patient about their symptoms and check for signs, including jaundice, abdominal swelling, or lumps.
Blood tests
Specific blood tests can measure liver function, specifically measuring the blood for a protein called Bilirubin. Bilirubin is made in the liver, stored in the gallbladder, makes up bile and is created when red blood cells are broken down. When bilirubin builds up, it causes the yellowish appearance in jaundice, and when bilirubin and other liver enzymes, such as alkaline phosphatase in the blood, are higher than normal, this can indicate damage which may be caused by cholangiocarcinoma.
Specific tumour markers
Blood tests may also include specific markers that correlate to certain cancers. Tumour markers are signals that are typically made by cancer cells and released into tissues and blood. They act as a beacon to help doctors identify cancer processes occurring within the body that are associated with specific types of cancers. In the case of cholangiocarcinoma, cancer markers called carcinoembryonic antigen and CA 19-9 can be requested, and if these are higher than the normal range, this can indicate cholangiocarcinoma.
Diagnostic Imaging may include:
Magnetic resonance cholangiopancreatography (MRCP) is a more specific type of imaging scan that collects detailed images of the liver, gallbladder, bile ducts and pancreatic duct.
Biopsy
A definitive way to diagnose cholangiocarcinoma is with a biopsy, whereby a piece of the liver, gallbladder or bile ducts is removed, and the cells are studied under a microscope to check for changes within the cells that may be cancerous.
What are the stages of cholangiocarcinoma?
The Tumour Node Metastasis (TNM) staging system is used for cholangiocarcinoma and can be broken down into the following, as detailed by Cancer Research UK :
T = size of the tumour
N = if the cancer has spread to the nearby lymph nodes
M = describes if the cancer spread to other parts of the body
Using these three markers, doctors use numbers against each of the letters to figure out the severity of the cancer.
Staging for cholangiocarcinoma
Intrahepatic bile duct cancer
- Stage 1: The tumour has grown in the intrahepatic bile duct.
- Stage 2: 1 or more tumours may have spread outside the intrahepatic bile duct to blood vessels.
- Stage 3: The tumour may have spread outside the liver to nearby organs and lymph nodes.
- Stage 4: The tumour has spread to other distant parts of the body, e.g., bone and lungs.
Perihilar bile duct cancer
- Stage 1: The tumour has grown in the tissue of the perihilar (common bile duct).
- Stage 2: The tumour has grown and may have spread to the nearby tissue.
- Stage 3: The tumour may have spread to the nearby lymph nodes and blood vessels around the liver.
- Stage 4: The tumour may have spread to multiple lymph nodes and distant organs, e.g., abdomen and bones.
Distal bile duct cancer
- Stage 1: The tumour forms in the distal bile duct.
- Stage 2: The tumour spread to more than 5 millimetres of the distal bile duct and nearby lymph nodes.
- Stage 3: The tumour has spread to multiple lymph nodes and the large blood vessels that carry blood to the stomach.
- Stage 4: The tumour has spread to distant parts of the body, e.g., the liver and stomach.
How is cholangiocarcinoma treated?
The 5-year survival rates for the different types of cholangiocarcinoma are reported to range from 2% to 15% for intrahepatic cholangiocarcinoma and from 2% to 30% for extrahepatic cholangiocarcinoma.8 Therefore, early detection and treatment are extremely important to the prognosis of cholangiocarcinoma.
The current European Society for Medical Oncology (ESMO) guidelines (2022),9 outlines the following treatment options for biliary tract cancers.
Surgery
Whenever possible, doctors will remove the tumour(s) and affected lymph nodes through surgery. This surgery may also include draining the bile ducts, and doctors may use a technique to redirect blood from the large vein of the liver (portal vein) into another part of the liver so that healthy sections of the liver may be spared during surgery.9
For distal bile duct cancer, the head of the pancreas may be removed alongside the cancerous bile duct, followed by reconstruction of the stomach.9
Chemotherapy after surgery
The use of chemotherapy after surgery has had mixed results; however, secondary analyses from the BILAP study suggested that capecitabine was associated with an improved overall survival of patients (53 months) compared to patients who were not given capecitabine (36 months).10
Therefore, ESMO recommends that this be considered for suitable patients after surgery.9
Patients who cannot have surgery
Some patients may have complications that make them unable to have surgery, such as liver cirrhosis, or patients who already had surgery but the cholangiocarcinoma has returned.9 In these cases, treatments include ablation, whereby radio waves or extreme heat or cold are used to promote cell death.11 In these cases, radiotherapy may also be recommended.9
Advanced disease
ESMO recommends chemotherapy as the standard of care for patients with advanced bile duct tumours that have spread to other parts of the body.9
The knowledge of specific genetic mutations in different cancers is increasing, meaning genetic testing is more widely available. This can offer hope for new directed therapies and precision medicines to be used on specific gene mutations patients may have.
Some of the directed therapies recommended by ESMO include:9
| Medicine | Specific genetic mutation |
| Ivosidenib | CCA and IDH1 mutations |
| FGFR inhibitors | FGFR2 mutations |
| Pembrolizumab | MSI-H/dMMR mutations |
| Dabrafenib–trametinib | BRAFV600E mutations |
| PARP inhibitors | BRCA1/2 or PALB2 mutations |
| NTRK inhibitors | NTRK fusions |
What support is available for patients and caregivers?
Facing a diagnosis of cholangiocarcinoma can be extremely overwhelming. However, there are several support groups and charities dedicated to giving you helpful information and support throughout. Some of these charities include:
Summary
Cholangiocarcinoma (which is also known as bile duct cancer) is a rare type of cancer that develops in the bile ducts. Bile ducts are the tubes that store bile (a substance that helps us break down fat from our food), which is produced in the liver. The bile ducts also transport bile from the liver to the small intestine.
Cholangiocarcinoma is broken down into 3 types:
- Intrahepatic
- Perihilar (extrahepatic)
- Distal (extrahepatic)
There are several risk factors; however, the majority cause inflammation, reduced flow of bile or total bile obstruction in the bile ducts that particularly predispose individuals to cholangiocarcinoma.
Diagnosis may include imaging scans, blood tests, and biopsies. Treatment options vary depending on the stage and location of the cancer but may include surgery, chemotherapy, radiation therapy and ablation, or directed therapies depending on the specific genes affected by cholangiocarcinoma.
Because of the relatively low 5-year survival rates for cholangiocarcinoma patients, early detection and treatment are vital for improving the treatment outcomes.
References
- Dave HD, Shumway KR, Al Obaidi NM. Physiology, biliary. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Aug 24]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK537107/
- Hundt M, Basit H, John S. Physiology, bile secretion. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Aug 11]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK470209/
- Mala A, Foteinogiannopoulou K, Koutroubakis IE. Solid extraintestinal malignancies in patients with inflammatory bowel disease. World J Gastrointest Oncol [Internet]. 2021 Dec 15 [cited 2023 Aug 24];13(12):1956–80. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8713323/
- Labib PL, Goodchild G, Pereira SP. Molecular pathogenesis of cholangiocarcinoma. BMC Cancer [Internet]. 2019 Feb 28 [cited 2023 Aug 24];19(1):185. Available from: https://doi.org/10.1186/s12885-019-5391-0
- Prueksapanich P, Piyachaturawat P, Aumpansub P, Ridtitid W, Chaiteerakij R, Rerknimitr R. Liver fluke-associated biliary tract cancer. Gut Liver [Internet]. 2018 May [cited 2023 Aug 24];12(3):236–45. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5945254/
- Brindley PJ, Bachini M, Ilyas SI, Khan SA, Loukas A, Sirica AE, et al. Cholangiocarcinoma. Nat Rev Dis Primers [Internet]. 2021 Sep 9 [cited 2023 Aug 24];7(1):1–17. Available from: https://www.nature.com/articles/s41572-021-00300-2
- Banales JM, Marin JJG, Lamarca A, Rodrigues PM, Khan SA, Roberts LR, et al. Cholangiocarcinoma 2020: the next horizon in mechanisms and management. Nat Rev Gastroenterol Hepatol [Internet]. 2020 Sep [cited 2023 Aug 24];17(9):557–88. Available from: https://www.nature.com/articles/s41575-020-0310-z
- Shroff RT, Kennedy EB, Bachini M, Bekaii-Saab T, Crane C, Edeline J, et al. Adjuvant therapy for resected biliary tract cancer: asco clinical practice guideline. JCO [Internet]. 2019 Apr 20 [cited 2023 Aug 24];37(12):1015–27. Available from: https://ascopubs.org/doi/10.1200/JCO.18.02178
- Gastrointestinal cancers | esmo [Internet]. [cited 2023 Aug 24]. Available from: https://www.esmo.org/guidelines/guidelines-by-topic/gastrointestinal-cancers/biliary-tract-cancer
- Primrose JN, Fox RP, Palmer DH, Malik HZ, Prasad R, Mirza D, et al. Capecitabine compared with observation in resected biliary tract cancer (Bilcap): a randomised, controlled, multicentre, phase 3 study. Lancet Oncol. 2019 May;20(5):663–73. Available from: https://www.thelancet.com/journals/lanonc/article/PIIS1470-2045(18)30915-X/fulltext
- Jarosova J, Macinga P, Hujova A, Kral J, Urban O, Spicak J, et al. Endoscopic radiofrequency ablation for malignant biliary obstruction. World J Gastrointest Oncol [Internet]. 2021 Oct 15 [cited 2023 Aug 24];13(10):1383–96. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8529920/




