 Medical contributor:
Medical contributor: First revision:
First revision: Pregnancy is a transformative and beautiful journey that brings joy, anticipation and wonder. However, this journey might occasionally be difficult if you have placenta previa.
Placenta previa is a medical condition during pregnancy where the placenta either entirely or partially restricts the baby's exit from the vagina. Managing the condition needs thorough understanding. Most people having placenta previa recover to give birth to healthy babies.
Placenta previa is a condition that necessitates a thorough study and specific delivery strategies. Let's endeavour to assist the birthing parents with education and support throughout their pregnancy experience as we explore the different aspects of this ailment.
Introduction to placenta previa
A placenta previa is an obstetric issue that manifests as painless vaginal bleeding in the third trimester due to an abnormal location of the placenta, close to or covering the internal cervical os (the opening of the womb).
Placenta previa can raise the birthing parent's risk for placenta accreta spectrum (PAS). Placenta accreta, increta, and percreta fall under this range of disorders. Uncontrolled postpartum haemorrhage (bleeding following delivery) caused by PAS or placenta previa may require a blood transfusion, a hysterectomy that renders the patient infertile, admission to the intensive care unit (ICU), or possibly result in death. Placenta previa affects 0.3% to 2% of third-trimester pregnancies, and has led to an increase in the rate of caesarean deliveries.
Placenta previa affects 5.2 out of every 1000 pregnancies worldwide. Worldwide, Asian-assigned females at birth (AFAB) had the highest prevalence, with an average incidence of 12.2 per 1000 pregnancies. It's debatable to what extent race affects placenta previa. A history of caesarean birth raises the risks by 1.5–5 times. According to a meta-analysis, the prevalence of placenta previa rises with the number of caesarean deliveries, from 1% after one to 2.8% after three to 3.7% after five deliveries. Maternal age is associated with a higher incidence of placenta previa. After ages 35 and 40, there is reportedly a 2% to 5% occurrence of placenta previa, a 9-fold increase over AFAB under 20.1,2
Causes and types of placenta previa
Although the exact cause of placenta previa is not always known, some variables may play a role in its occurrence. The primary causes and risk factors are as follows:
- Uterine Abnormalities: endometrial scarring and uterine abnormalities are associated with an increased risk of placenta previa. A zygote's (fertilised egg) implantation requires a collagen and oxygen-rich environment. The outer layer of the zygote (the blastocyst) forms the placenta. Old uterine scars offer a collagen and oxygen-rich environment therefore the placenta may implant and cover the cervical os or invade the walls of the myometrium
- Maternal age beyond 35 (advanced maternal age): increasing maternal age is associated with an increased likelihood of placenta previa, possibly related to increased rates of atherosclerosis which reduce blood supply to the uterus and placenta
- Multiparity (multiple pregnancies at a time) and the use of assisted reproductive technology (ART)
- Prior caesarean section history: endothelial lining damage and uterine scarring may be the cause. The placenta's affinity and adherence to the caesarean scar may also affect implantation of future pregnancies
- Smoking and cocaine use: cigarette smoke contains combined nicotine and carbon monoxide, which have strong vasoconstrictor effects on placental vessels (making them constrict and narrow), therefore reducing placental blood flow, which results in improper placentation
- History of dilatation and curettage (D&C): a threefold increased risk of placenta previa was recorded in AFAB who had previously undergone uterine dilatation and curettage
- A history of placenta previa can also be a substantial risk factor for placenta previa in subsequent pregnancies1,3
Created by Deepika Rana1,4
Symptoms and complications
The most common signs of placenta previa include sudden, painless vaginal bleeding after 20 weeks of pregnancy. Blood may be a bright red colour. The life of the birthing parent and the unborn child may be at risk if the bleeding becomes severe. Some people AFAB have moderate abdominal, belly and back cramps or contractions.
The following table summarises placenta previa complications in neonates/infants and birthing parents.
| Neonates/infants | Maternal complications |
| The foetus can be in an unusual position and not grow as normally would be expected (intrauterine growth restriction) | Postpartum haemorrhage including rebleeding (in cases of placenta previa, placenta accreta, increta and percreta, planning birth and controlling haemorrhage are crucial) |
| The membranes around the foetus may rupture soon (premature rupture of membranes) | Higher rates of blood transfusion |
| The cervix's opening blocked by blood arteries that connect the placenta and umbilical cord (vasa previa) | Placental abruption |
| Congenital abnormalities,foetal anaemia and Rh isoimmunisation | Preterm delivery |
| Low birth weight (< 2500 g) and jaundice | An increase in postpartum endometritis incidence |
| Neonatal respiratory distress syndrome (NRDS) | Uterine bleeding and, the complication of disseminated intravascular coagulopathy (DIC) serves almost all cases in the United States, wherein the maternal death rate is 0.03%. |
| An extended hospital stay with admission to the neonatal intensive care unit (NICU) | |
| Neuro-developmental lapses and sudden infant death syndrome (SIDS) is more common in infants | |
| The death rate for newborns in the United States can reach 1.2% |
Diagnosis
Medical history and symptoms
The doctor will ask about any symptoms you may be experiencing, especially in the second and third trimesters of pregnancy, such as vaginal bleeding. It's vital to be specific regarding the occurrence, amount, and accompanying pain.
Physical examination
The positioning of the placenta and cervix is determined by pelvic examination. The likelihood of substantial bleeding means that a cautious and attentive approach is required during this inspection.
Ultrasound
Ultrasound imaging is a standard diagnostic tool. Transvaginal ultrasound is helpful for patients with posterior placenta previa since it increases diagnostic clarity, takes less time to scan, and doesn't increase the risk of haemorrhaging (bleeding). Since the cervix and lower uterine segment are closer to the vaginal probe transducer, higher-frequency ultrasound waves improve resolution and allow for a more precise assessment of the relationship between the placental edge and the internal os.5
Transabdominal ultrasonography can diagnose placenta previa with an accuracy of up to 95% and a 7% false-negative rate. Maternal obesity, acoustic shadowing of the foetal head in a cephalic presentation, failure to find the internal cervical os (which is crucial for correct diagnosis), trouble imaging a posterior placenta, and lateral uterine walls can all harm the accuracy of the test. Furthermore, a full maternal bladder, essential during transabdominal ultrasound imaging, may result in a false-positive diagnosis if the bladder is too distended. In this case, the cervix would appear unnaturally extended and give a regularly inserted placenta the appearance of encroachment into the interior cervical os.
Transperineal sonography (TPUS) is a valuable method in addition to transabdominal studies. In these situations, sonography calls for visualising the cervix and the inferior edge of the placenta. The cervix is virtually always visible on transperineal sonograms, while the placenta's lower edge remains hidden. Transabdominal sonograms allow visualisation of the placenta's bottom edge in certain circumstances.6
Management and treatment
The management and treatment of placenta previa depends on the condition's severity, the foetus' gestational age, and the birthing parent’s, and the child's, overall health. A step-by-step process exists to treat vaginal bleeding throughout the third trimester. The following are some general principles:
- Monitoring
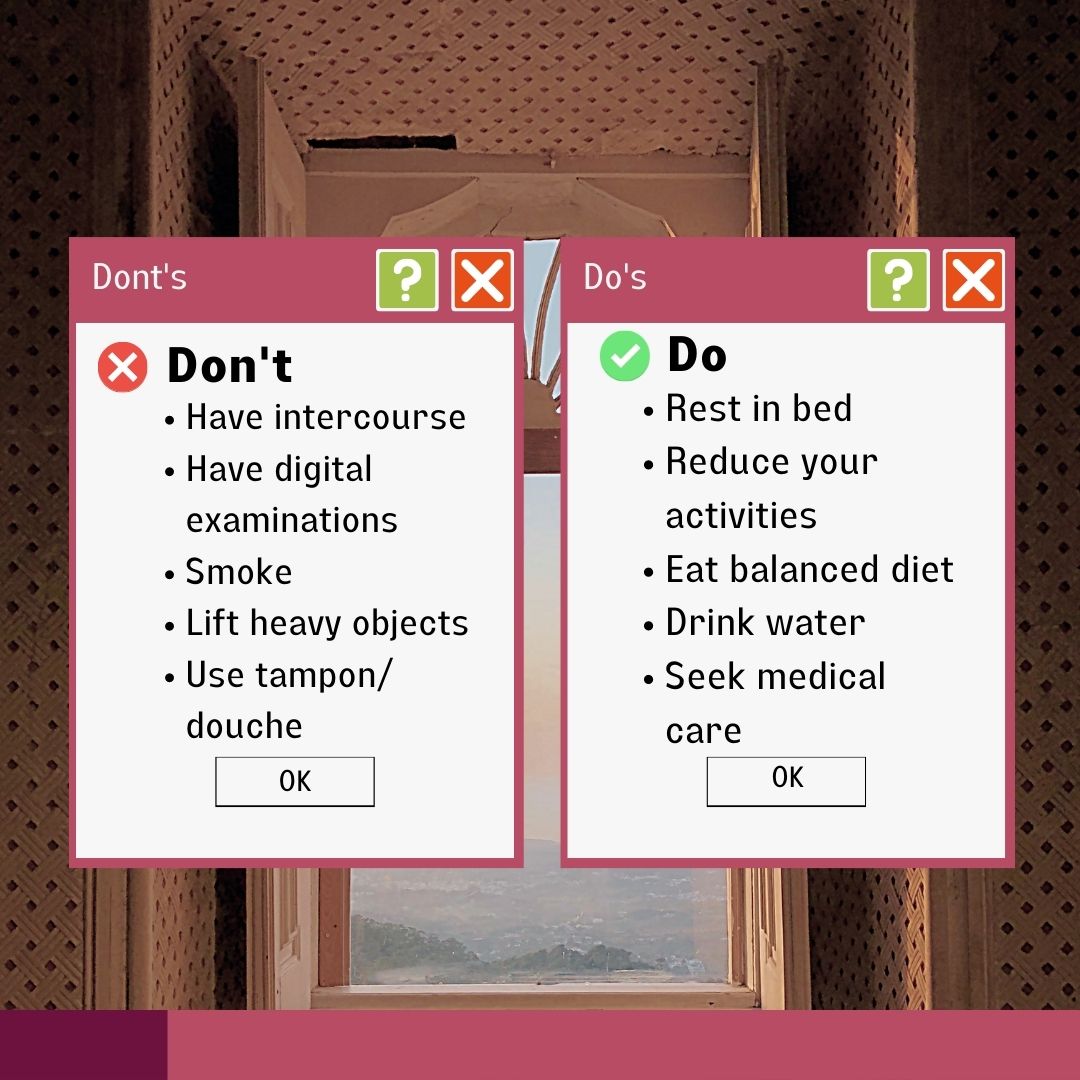
After a diagnosis, close observation is necessary to monitor bleeding and the placenta's placement. It is best to stay in bed if bleeding develops.
- Blood transfusion
In the labour and delivery unit an individual is evaluated with the welfare of the foetus and the birthing parent as the primary focus. To ascertain haemoglobin (Hg) levels and the potential need to administer Rh immunoglobulin depending on the maternal Rh status, complete blood count (CBC) and type and screen testing (T&S) are submitted. If significant vaginal bleeding manifests during the evaluation, blood should be cross-matched to replace the lost volume. It is advised to initiate a massive transfusion protocol if bleeding occurs, two to four units of blood are required, and quick access to blood products is necessary.
- Hospitalisation
Individuals with recent vaginal bleeding and placenta previa should be admitted to the medical facility for close monitoring. Patients are monitored for at least 48 hours while an active bleeding scene happens. After the underlying bleeding scene has reduced with desirable foetal evaluation, it is appropriate to administer eager management to some patients at home.
The goal of administering tocolytic drugs is to reduce foetal morbidity and mortality. One study suggested that utilising tocolytics lengthens pregnancy and increases the baby's birth weight without having unfavourable effects on the birthing parent or the foetus. Bose et al.'s review article concluded that tocolysis beyond 48 hours is not clinically necessary and does not improve the perinatal outcome.
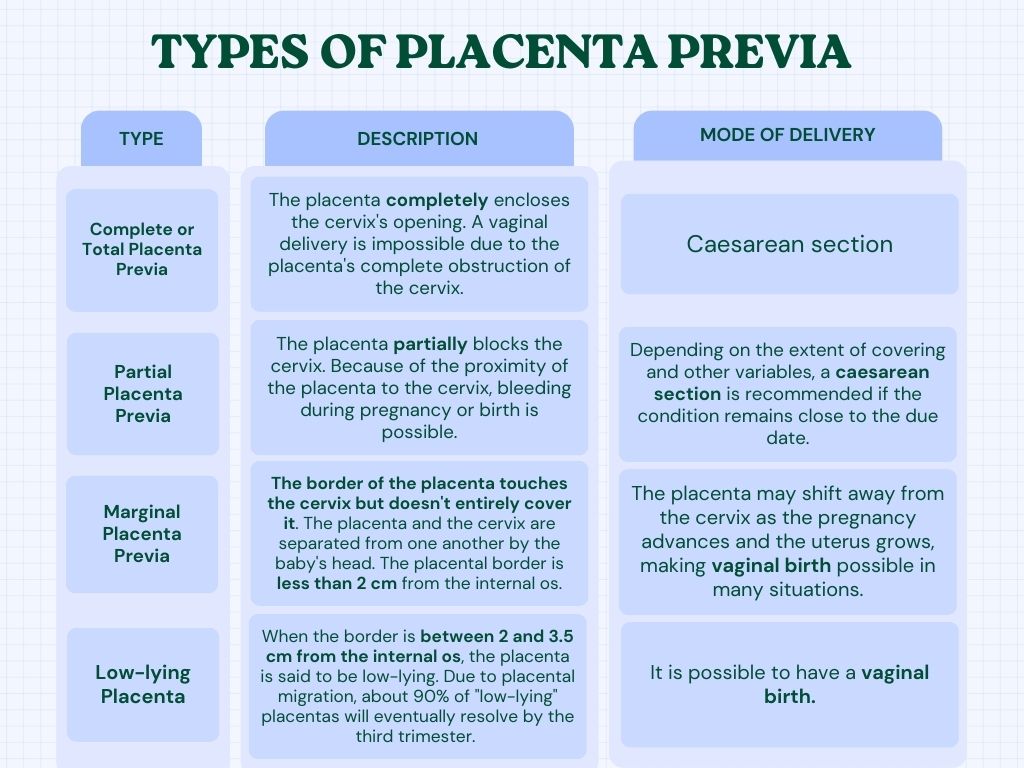
- Approach to delivery
The location of the placenta's edge with the cervix’s inner os determines the delivery technique. When the placenta is less than 2 cm from the inner os, prior studies advised elective caesarean delivery. In a review analysis of 121 pregnancies, 90% of pregnancies with a placental edge-to-cervical os separation of 1-2 cm resulted in caesarean deliveries.
- Surgical method
Delivery is recommended in the late preterm phase between 36 and 37 weeks of gestation in patients with uncomplicated placenta previa.
- Corticosteroids
If the gestational age is < 34 weeks, betamethasone injection should be administered as it promotes foetal lung maturity.
- Controlling blood loss
These complicated pregnancies need delivery plans that include patient-coordinated blood and informed consent for a potential caesarean hysterectomy. The following are some methods for preventing bleeding predelivery placement of balloon catheters for angiographic embolisation of pelvic vessels, aortic balloons, hypogastric artery ligation, uterine artery ligation (O'Leary stitch refers to stitching or suturing the uterine artery to stop bleeding or lessen blood flow to the uterus) and hysterectomy.7
FAQ
Are there any lifestyle changes or precautions to take with placenta previa?
Created by: Deepika Rana1
Is it possible to lower my risk of placenta previa?
Smoking and advanced maternal age are risk factors that can increase risk, but prevention is not possible.
Can placenta previa recur in subsequent pregnancies?
First-time caesarean deliveries are associated with higher chances of placenta previa and abruption in subsequent pregnancies. The probability of previa increases with more prior caesarean births, according to a dose-response pattern.8
When should I see the doctor?
When vaginal bleeding first appears, placenta previa can have severe consequences and necessitates prompt medical attention. An interdisciplinary team approach is required to provide the patient with the best care possible. Before vaginal bleeding, patients diagnosed with placenta previa should have several conversations with their gynaecologist about care and expectations.1
Summary
Most people with placenta previa recover and give birth to healthy children. Following the advice of your prenatal care provider, you're likely to have a safe delivery. Individuals who undergo routine prenatal care have this condition identified before the onset of symptoms. It enables the carer and birthing parent to decrease this condition's risks.
References
- Anderson-Bagga FM, Sze A. Placenta previa. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Jul 31]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK539818/
- Rowe T. JOGC. Journal of Obstetrics and Gynaecology Canada [Internet]. 2014 Aug [cited 2023 Jul 31]; 36(8):667–668. Available from: https://www.jogc.com/action/showPdf?pii=S1701-2163%2815%2930503-X
- Latif L, Iqbal UJ, Aftab MU. Associated Risk Factors of Placenta Previa A Matched Case-Control Study [Internet]. 2015 Oct-Dec [cited 2023 Jul 31];1344-1345 PJMHS Vol 9, No 4. Available from: https://pjmhsonline.com/2015/oct_dec/pdf/1344%20%20%20Associated%20Risk%20Factors%20of%20Placenta%20Previa%20A%20Matched%20Case%20Control%20Study.pdf
- Dashe MD JS. Toward consistent terminology of placental location - ScienceDirect [Internet]. ScienceDirect.com | Science, health and medical journals, full-text articles and books. Elsevier; 2013 [cited 2023 Aug 2]. Available from: https://www.sciencedirect.com/science/article/abs/pii/S0146000513000827?via%3Dihub
- Sherman SJ, Carlson DE, Platt LD, Medearis AL. Transvaginal ultrasound: does it help in the diagnosis of placenta previa?: Diagnosis of placenta previa. Ultrasound Obstet Gynecol [Internet]. 1992 Jul 1 [cited 2023 Aug 2];2(4):256–60. Available from: http://doi.wiley.com/10.1046/j.1469-0705.1992.02040256.x
- Hertzberg BS, Bowie JD, Carroll BA, Kliewer MA, Weber TM. Diagnosis of placenta previa during the third trimester: role of transperineal sonography. American Journal of Roentgenology [Internet]. 1992 Jul [cited 2023 Aug 2];159(1):83–7. Available from: https://www.ajronline.org/doi/pdf/10.2214/ajr.159.1.1609727
- Almnabri AA, Ansari EAA, Abdulmane MM, Saadawi DW, Almarshad TA, Banoun AA, et al. Management of Placenta Previa During Pregnancy. The Egyptian Journal The Egyptian Journal of Hospital Medicine [Internet]. 2017 Jul;[cited 2023 Aug 3]; Vol.68 (3), Page 1549-1553. Available from: https://ejhm.journals.ekb.eg/article_13638_25c4d0b9ed892b17af538114fa7a3fc6.pdf
- Getahun D, Oyelese Y, Salihu HM, Ananth CV. Previous cesarean delivery and risks of placenta previa and placental abruption. Obstetrics & Gynecology [Internet]. 2006 Apr [cited 2023 Aug 3];107(4):771. Available from: https://journals.lww.com/greenjournal/Abstract/2006/04000/Previous_Cesarean_Delivery_and_Risks_of_Placenta.6.aspx




