

What is endometriosis?
Endometriosis is a medical condition whereby tissue lining the uterus, the female reproductive organ, starts to grow elsewhere, for example, within the fallopian tubes or pelvic region. These growths cause the immune system to react, leading to inflammation and chronic pain. Endometriosis can develop at various stages of life, from when a person first reaches their reproductive age up until menopause.
What are the signs and symptoms of endometriosis?
Endometriosis can cause a range of symptoms that may vary from person to person in type and severity. The infographic below shows some of the most common symptoms:
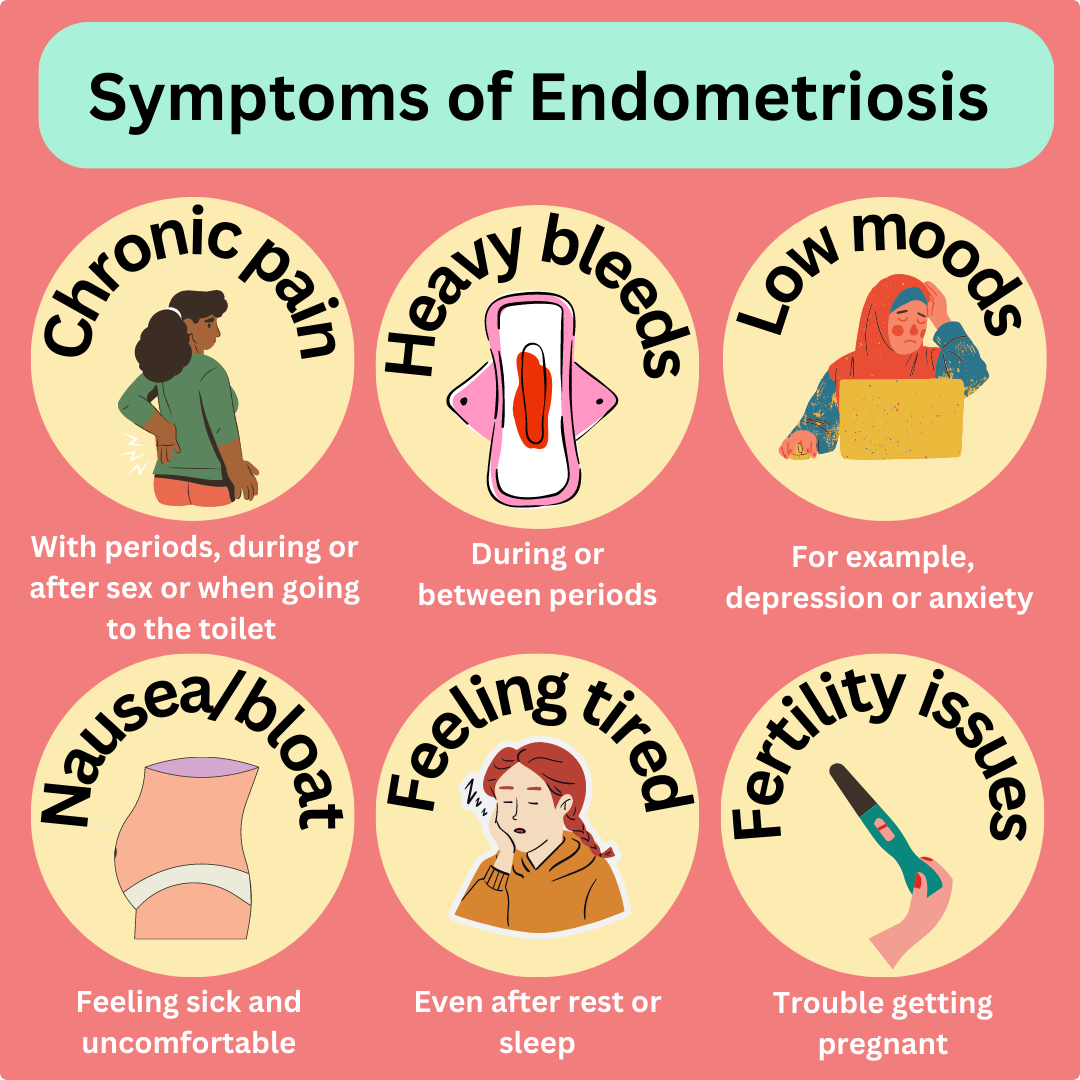
Image source: Parr-Reid S. Canva.
Although these symptoms are common in those with endometriosis, not all individuals living with endometriosis show symptoms.
What are the complications of endometriosis?
Due to symptoms such as chronic pain (linked to inflammation), as well as a lack of societal and clinical understanding of the condition, there are some complications a person will face. For example, chronic pain, tiredness, low moods, and infertility can lower a person’s quality of life. Pain may prevent people from attending school, work or other activities, leading to social isolation.
Pain during sex may lead to avoidance or disruption to sexual intercourse, affecting both those with endometriosis and their partners.
What causes endometriosis?
Research has yet to unveil the exact cause of endometriosis. However, some studies have looked into potential factors, such as faulty genes, problems with the immune system, and cells from the womb growing improperly.
Some theories may explain why endometriosis develops. For example, the theory of 'retrograde menstruation', where cells from the uterus lining move backwards towards the fallopian tube and settle outside of the uterus. It is also thought that some individuals who have surgery on their uterus may develop uterus cell growth around the incision area. And instead of white blood cells in the immune system destroying these cells, they become dysfunctional and don't remove them.
Who gets endometriosis?
Endometriosis is present in 10–15% of reproductive women, as well as 70% of those who live with chronic pelvic pain.1,2
The risk of developing endometriosis varies by ethnicity, with Asian people assigned female at birth (PAFAB) being most at risk. Black PAFAB are less likely to be diagnosed with endometriosis than white PAFAB. Hispanic PAFAB are less likely to be diagnosed than white PAFAB.
Some risk factors that increase the likelihood of being diagnosed with endometriosis are listed below:
- Having your first period at a younger age3,7
- Having short periods5,6,8,10
- Being tall7,11
- Drinking excessive amounts of alcohol12,14
- Drinking lots of caffeine15
These are only risk factors and not causes, and no single risk factor listed will result in a diagnosis of endometriosis.
How is endometriosis diagnosed?
When diagnosing endometriosis, a careful medical history and various methods can be used. The main diagnostic methods are described in the table below:
| Method of diagnosis | How it works |
| Laparoscopy | A surgical procedure where a doctor makes a small cut in the abdomen. A very thin camera is then inserted, and tissue near and including the uterus is examined to check for signs of abnormal tissue growth outside of the uterus |
| Biopsy | A surgical procedure where a doctor makes a small cut in the abdomen. A very thin camera is then inserted, and tissue near and including the uterus is examined to check for signs of abnormal tissue growth outside of the uterus. |
| Ultrasound | A non-surgical procedure where an ultrasound device is inserted into the vagina to use sound waves to visualise the pelvic area for signs of endometriosis |
| MRI | A non-surgical procedure where an MRI machine uses magnetic waves to visualise the pelvic region for signs of endometrial tissue growth outside of the uterus |
If you are worried about speaking with your healthcare provider, it can help to take a family member or friend with you to your appointment for support.
Whilst symptoms may first be present during adolescence, the average wait time between the onset of symptoms and diagnosis is 6.7 years. This is because endometriosis shows similar symptoms to those of other conditions, such as fibromyalgia, irritable bowel syndrome and ovarian cysts.16
How is endometriosis treated?
Whilst there is no cure for endometriosis, there are a variety of ways to manage pain in endometriosis, which you can discuss with your healthcare provider. Some of the main methods of managing endometriosis are shown in the infographic below:
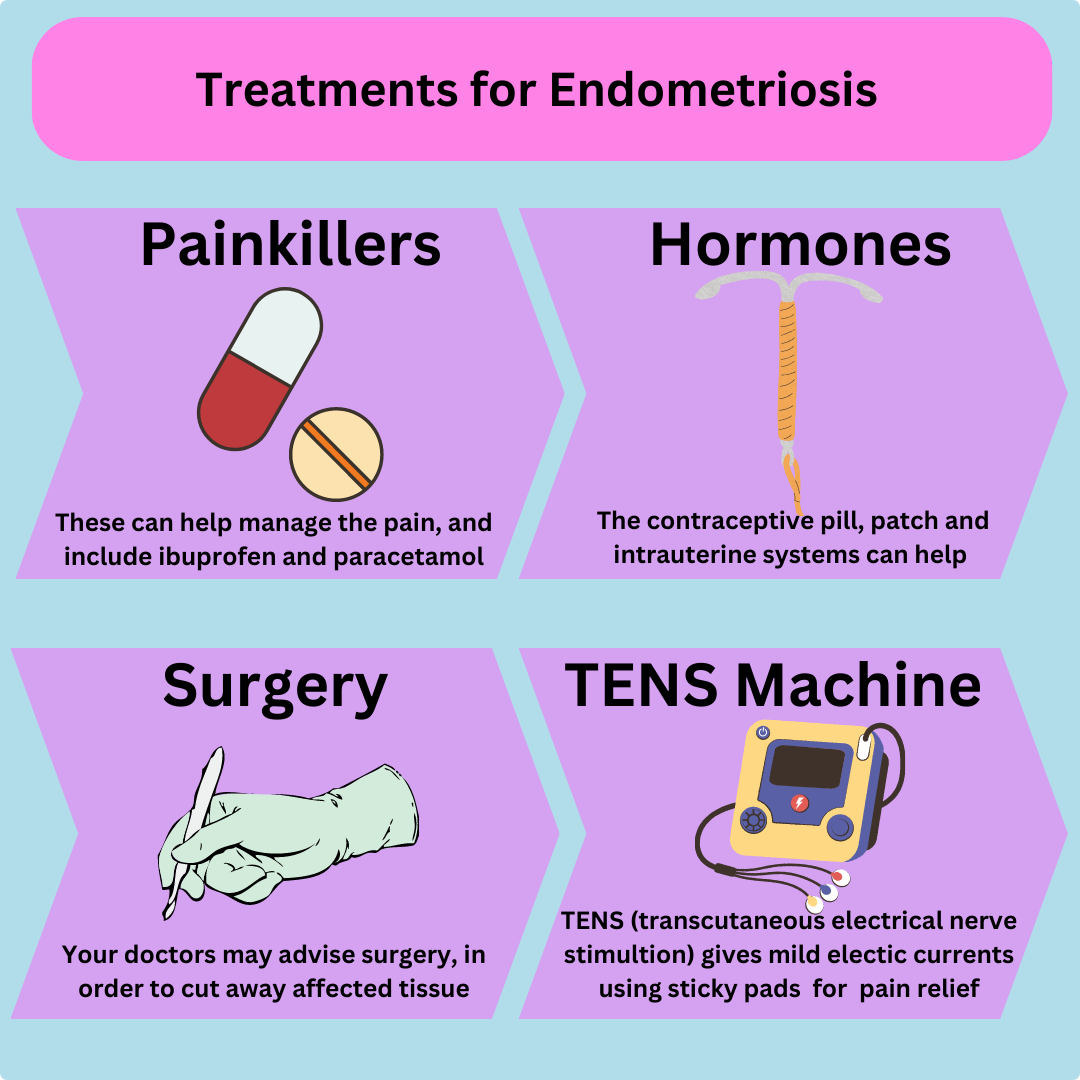
Image source: Parr-Reid S. Canva.
The purpose of contraceptive devices for treating endometriosis is to induce lighter periods by making the uterus lining thinner. The thinning of the lining is achieved via the use of the hormones oestrogen and progesterone. A thinner uterus lining decreases the chances of uterus tissue migration, hence lowering the chance of pain due to uterus tissue growing elsewhere. Please note that it is important to discuss the side effects and risks of contraceptives with your healthcare provider before committing to them.
It is important to remember that no single method of pain relief will necessarily work alone for treating endometriosis. So, it is worth discussing possible combinations of treatments with your healthcare provider. For example, TENS machines can only provide temporary pain relief, whereas hormone therapies can provide longer-term treatment.
How to support someone living with endometriosis?
Supporting someone with endometriosis can include providing arrangements at school or within the workplace to ensure that their pain is managed safely.
The Endometriosis Network Canada has some useful recommendations for how you can support someone with managing endometriosis whilst at school. Endometriosis UK also provides a useful PDF guide to workplace rights and accommodations for those living with endometriosis. In addition to this, the charity also provides support for those living with and affected by endometriosis through its helplines, online web chat, and support groups.
Day to day, it is important to ask the individual what they may need to support them rather than making any assumptions.
Tackling endometriosis stigma
Stigma about endometriosis can come from anyone, including medical professionals, which is why it is really important to speak up against it, as Kayleigh Honeyball, age 30, shares:
“I had a colonoscopy, too many ultrasounds to count, and they removed my appendix to rule out that as a cause of pain. My gynaecologist told me it was muscular, then irritable bowel syndrome, and then stress. Sometimes, I wondered if they thought I was making it up.”
It took Kayleigh six years to get a diagnosis; undoubtedly, it was a time filled with uncertainty as well as chronic pain.
Kayleigh’s endometriosis also impacted her pregnancy:
“I watched everyone around me start families, and we had no luck. At 22, I nearly lost my ovary due to an 8 cm cyst. Then, at 23, after experiencing a miscarriage and extreme pain, I went to A&E, and the nurse did a pregnancy test, and I found out we were pregnant and the baby was healthy, which was such a relief!”
The Endometriosis Foundation 2023 campaign ‘Our Fertility Matters’ aims to tackle stigma relating to infertility in those living with endometriosis.
In the US, a yearly ‘Worldwide EndoMarch’ takes place to raise awareness about endometriosis as well as garner support for better policies supporting those with endometriosis.
March is Endometriosis Awareness Month, where people across the globe fundraise, share their stories, lobby their MPs or congress members to better support those with endometriosis, and share information about endometriosis on social media.
Summary
Endometriosis is a condition where the tissue that normally grows in the lining of the uterus also starts to grow in other parts of the body, such as the fallopian tubes or pelvic region. This abnormal growth causes the surrounding tissue to become inflamed as the immune system tries to prevent the tissue growth. This inflammation causes pain, which can be chronic.
Around 10-15% of people who are of reproductive age will be diagnosed with endometriosis. Not all people diagnosed with the condition experience symptoms, but if they do, they may experience pain, tiredness, heavy periods, pain during or after sex or going to the toilet, and low moods. Endometriosis is diagnosed through a sample of the abnormal tissue that may be studied in a lab using a biopsy, or a camera may be inserted into the abdomen to look at the tissues around the uterus. Whilst there is no cure for endometriosis, it can be managed using pain relief medications, surgery, hormone therapies, or other methods of pain relief.
References
- Giudice LC and Kao LC. Endometriosis. Lancet 2004;364(9447): 1789–1799. https://pubmed.ncbi.nlm.nih.gov/15541453/
- Carter JE. Combined hysteroscopic and laparoscopic findings in patients with chronic pelvic pain. J Am Assoc Gynecol Laparosc 1994;2: 43–47. https://pubmed.ncbi.nlm.nih.gov/9050532/
- Missmer SA, Hankinson SE, Spiegelman D, Barbieri RL, Marshall LM and Hunter DJ. Incidence of Laparoscopically Confirmed Endometriosis by Demographic, Anthropometric, and Lifestyle Factors. Am J Epidemiol 2004;160(8): 784–96. https://pubmed.ncbi.nlm.nih.gov/15466501/
- Darrow SL, Vena JE, Batt RE, Zielezny MA, Michalek AM and Sharon S. Menstrual Cycle Characteristics and the Risk of Endometriosis. Epidemiology 1993;4(2): 135–142. https://pubmed.ncbi.nlm.nih.gov/8452902/
- Matallioakas I, Cakmak H, Fragouli Y, Goumenou A, Mahutte N and Arici A. Epidemiological characteristics in women with and without endometriosis in the Yale series. Arch Gynecol Obstet 2008;277(5): 389–393. https://pubmed.ncbi.nlm.nih.gov/17922285/
- Missmer S. Hankinson S, Spiegelman D, Barbieri R, Malspeis S, Willett W and Hunter D. Reproductive history and endometriosis among premenopausal women. Obstet Gynecol 2004;104(5): 965–974. https://pubmed.ncbi.nlm.nih.gov/15516386/
- Signorello LB, Harlow BL, Cramer DW, Spiegelman D and Hill JA. Epidemiologic determinants of endometriosis: a hospital-based case-control study. Ann Epidemiol 1997;7(4): 267–274. https://pubmed.ncbi.nlm.nih.gov/9177109/
- Moen MH and Schei B. Epidemiology of endometriosis in a Norwegian county. Acta Obstet Gynecol Scand 1997;76(6): 559–562. https://pubmed.ncbi.nlm.nih.gov/9246963/
- Cramer DW, Wilson E, Stillman RJ, Berger MJ, Belisle S, Schiff I, Albrecht B, Gibson M, Stadel BV and Schoenbaum SC. The relation of endometriosis to menstrual characteristics, smoking, and exercise. JAMA 1986;255(14): 1904–1908. https://pubmed.ncbi.nlm.nih.gov/3951117/
- Sangi-Haghpeykar H and Poindexter AN. Epidemiology of endometriosis among parous women. Obstet Gynecol 1995;85(6): 983–992. https://pubmed.ncbi.nlm.nih.gov/7770271/
- Hediger ML, Hartnett HJ, Buck Louis GM. Association of endometriosis with body size and figure. Fertil Steril 2005;84(5): 1366–1374. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1343487
- Parazzini F, Chiaffarino F, Surace M, Chatenoud L, Cipriani S, Chiantera V, Benzi G and Fedele L. Selected food intake and risk of endometriosis. Hum Reprod 2004;19(8): 1755–1759. https://pubmed.ncbi.nlm.nih.gov/15254009/
- Grodstein F, Goldman MB and Cramer DW. Infertility in women and moderate alcohol use. Am J Public Health 1994;84(9): 1429-1432. https://pubmed.ncbi.nlm.nih.gov/8092366/
- Heilier JF, Donnez J, Nackers F, Rousseau R, Verougstraete V, Rosenkranz K. Environmental and host-associated risk factors in endometriosis and deep endometriosis nodules: a matched case-control study. Environ Res 2007;103(1)121–129. https://pubmed.ncbi.nlm.nih.gov/16781705/
- Grodstein F, Goldman MB, Ryan L and Cramer DW. Relation of female infertility to consumption of caffeinated beverages. Am J Epidemiol 1993;137(12): 1353–1360. https://pubmed.ncbi.nlm.nih.gov/8333416/
- Nnoaham KE, Hummelshoj L, Webster P, d’Hooghe T, de Cicco Nardone F, Kenkinson C, Kennedy SH and Zondervan KT. Impact of endometriosis on quality of life and work productivity: a multicenter study across ten countries. Fertil Steril 2011;96(2): 366–373. https://pubmed.ncbi.nlm.nih.gov/21718982/




