


Introduction
Did you know according to Cancer Research UK, there were 18.1 million new cases of cancer worldwide in 2020? By 2040, there will be 28 million new cases annually worldwide. The UK has a greater incidence rate than 90% of other countries. Observing World Cancer Day (4th of February every year) is to raise awareness of cancer as a disease of public health and strengthen efforts to increase access to screening, early detection, treatment, and palliative care.
Uncontrolled cell growth that can spread to surrounding tissue and throughout the body is termed cancer. Radiation therapy and chemotherapy serve to treat cancer. Chemotherapy kills rapidly proliferating cells by infusing potent medications into the body. Radiation therapy eliminates cancer cells by using radiation.
As we continue to learn about the distinctions between chemotherapy and radiation therapy, explore the complicated world of cancer treatment by reading this article.
Cancer treatment options
Treatment options and outcomes vary by the type of cancer, origin, and stage of progression. The most common and conventional forms of treatment include radiotherapy, chemotherapy, and surgery. Modern treatment approaches include:
Ionising radiation is the type of radiation utilised in therapy that transfers energy from the rays to the body's cells by passing particles in biological bodies to charge electrically upon incidence. This energy either directly destroys cancer cells or genetically modifies them to allow cell death.
Chemotherapy stops the growth of tumours by preventing them from dividing and leading to apoptosis. Various individuals exhibit distinct protein expression patterns in their tumours and have unique underlying genetic causes.
Precision and personalised medicine (PPM) is a rapidly expanding discipline that analyses and alters patient genetic data to enable the development of tailored treatments for each unique subtype of cancer.1,3
Radiation therapy
Definition and mechanism
Utilising targeted X-rays or subatomic particles primarily for cancer care in curative and palliative contexts is known as radiation therapy. It can be delivered internally or externally. The most popular type of radiation therapy, known as "teletherapy”, or external beam radiotherapy (EBRT), uses a radioactive source outside the patient and directs its energy towards the target of interest. The process of concentrating naturally occurring radioactive sources that gradually decay and provide high radiation doses in a specific location is known as brachytherapy.4
High-energy radiation damages cells' genetic material (deoxyribonucleic acid - DNA), preventing further cell division and proliferation (the rapid growth of cells). The image below shows two ways radiation therapy eliminates cancer cells.
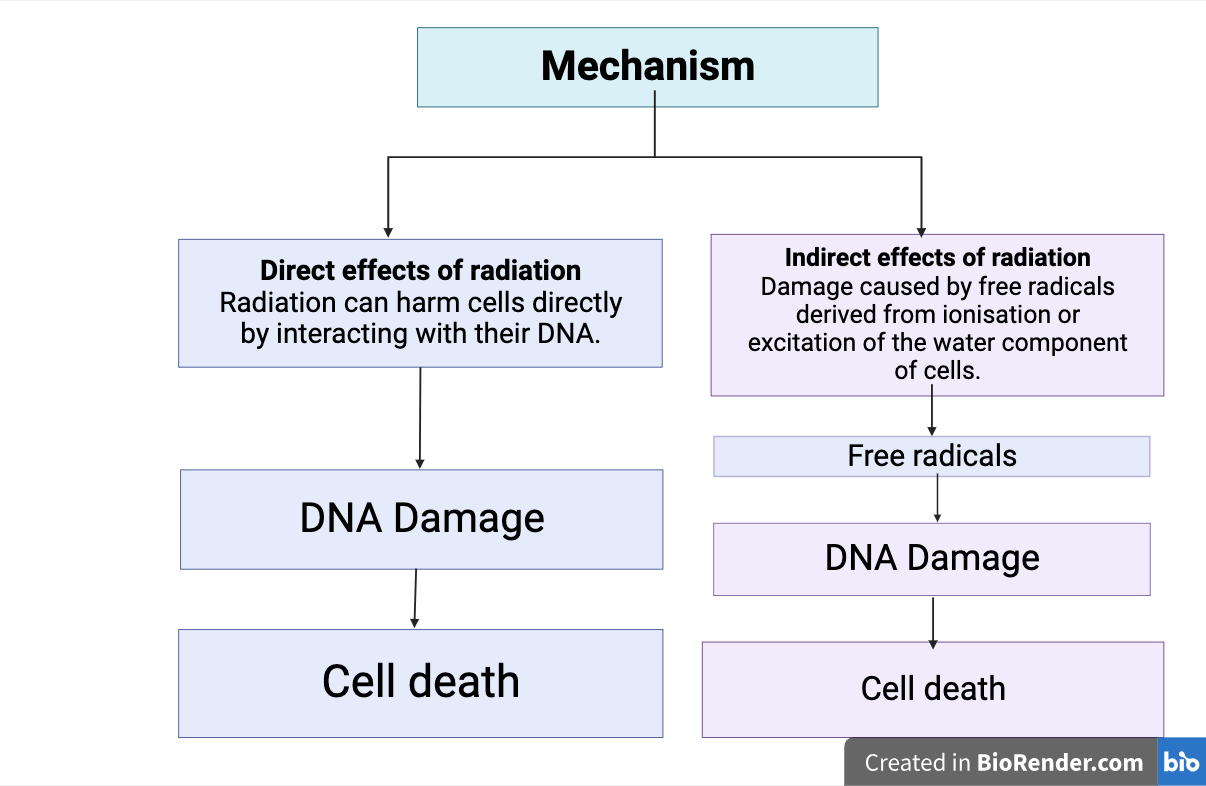
Created by: Deepika Rana (Created with BioRender.com)
Different forms of cell death (apoptosis, mitotic catastrophe, necrosis, senescence and autophagy) occur through radiation therapy to produce its therapeutic impact. Before cancer cells begin to die, treatment may last for hours, days, or weeks. Once radiation therapy is over, cancer cells may continue to die for weeks or months.2
Indications and targeted areas
Table 1 displays several malignancies treated with radiation therapy.

Table 1: Cancers that can be treated with radiation therapy (skin cancer, prostate, lung, cervix, breast cancer, rectal, anal, and endometrial carcinoma and Hodgkin’s lymphoma.2
Created by: Deepika Rana (Created with BioRender.com)
Radiotherapy's successful execution depends on the definition of the tumour and target volumes. Radiotherapy planning requires diagnostic imaging, as well as assistance and guidance from professionals. It involves three main volumes:
- Gross tumour volume (GTV) — it is the location and size of the gross tumour and what is visible, palpable, or imaged.
- Clinical target volume (CTV) — includes the GTV plus a margin for sub-clinical disease spread that is not fully imageable.
- Planned target volume (PTV) — it is a geometric idea intended to guarantee that the dose of radiation therapy reaches the CTV. Radiotherapy planning should consider critical tissue structures termed organs at risk (ORs).5
Procedure and sessions
A simulation session is the initial step for EBRT. Imaging techniques (CT or MRI) help to landmark the patient's position, and immobilisation on the treatment table using several devices (thermoplastic shells, wedges, bite blocks) are all part of this process. A treatment plan specifying the volume of tissue treated, the dose administered, and the number of fractions needed to deliver this dose follows in order by radiation oncologists and physicists.
In a technique called conformal radiotherapy, radiation beams are administered from many directions to fit the target volume as closely as possible, maximising the dose to the target and minimising exposure of normal tissue. Treatments with external beam radiation frequently occur in fractions of a day, Monday through Friday, and are administered twice a day or once a week. The treatment takes a few minutes, but overall positioning requires 15 to 30 minutes. The dosage of a curative regimen is between 40 and 80 Gray (Gy), spread out over three to eight weeks.6
Side effects and risks
Table 2 below lists side effects and potential complications.
| Acute effects | Potential Complications |
| Fatigue | Late malignancy |
| Sunburned skin appearance with ulceration and bleeding (rare) | Hair loss, telangiectasia and tanning |
| Cough | Fibrosis, coronary artery disease (CAD) and pericarditis |
| Mucositis Xerostomia Dysphagia Weight loss Anorexia | Osteonecrosis of the mandible, dental issues and oesophageal perforation (rare) |
| Diarrhoea, nausea and vomiting | Chronic bowel change, rectal urgency and fistulas |
| Headache, seizures, and sexual dysfunction | Infertility6 |
Table 2: Side effects and potential complications of radiotherapy
Chemotherapy
Definition and mechanism
Chemotherapy, most commonly used for cancer treatment, is a drug-based approach that stops or slows down the proliferation of cells. It works in conjunction with other therapies like radiation or surgery.
Chemotherapy inhibits the growth of tumours by preventing them from dividing and apoptosis. The body's normal biological processes remove damaged or excess cells from the body, allowing new cells to proliferate. Cancer cells are immortal as they are not susceptible to apoptosis. Consequently, in malignant masses, the ratio of cell proliferation to cell death is high, in contrast to healthy bodies where cell proliferation is balanced and regulated by cell death.
The two categories of chemotherapeutic medications are cytostatic and cytotoxic drugs, respectively.1,7 The image below displays different kinds of chemotherapy medications (alkylating agents, antimetabolites, anthracyclins, mitotic and topoisomerase inhibitors and hormone therapy).1
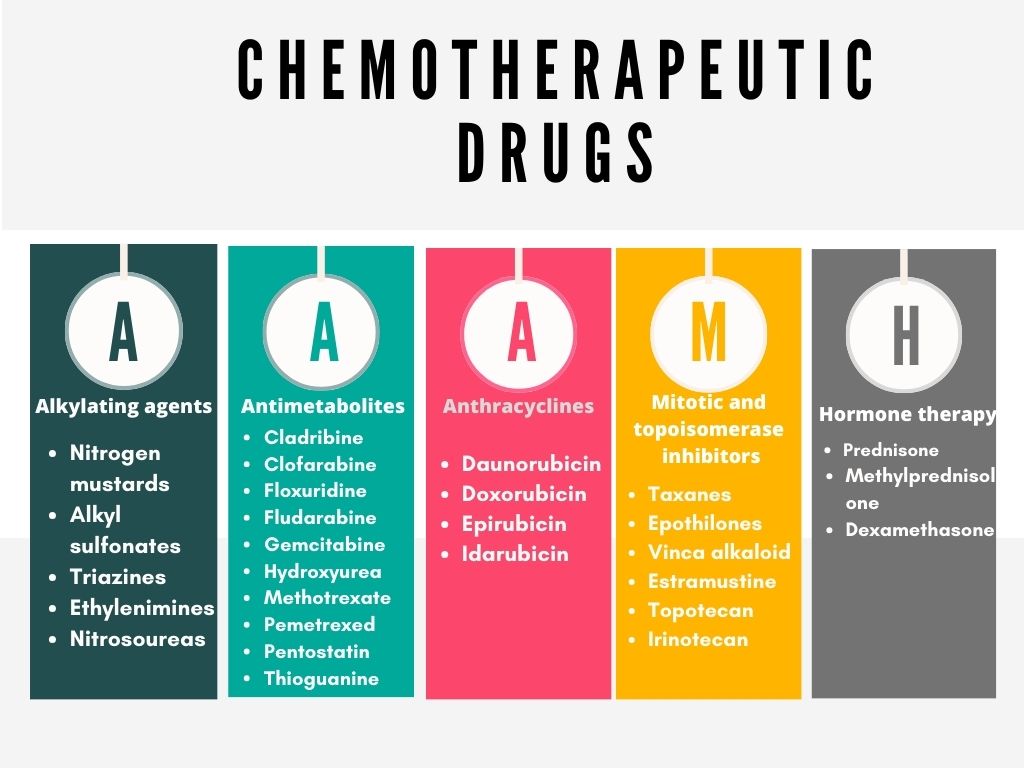
Created by: Deepika Rana (Canva)
Significance and suitability
Chemotherapy is given in combined, metastatic, neoadjuvant, and adjuvant conditions. Neoadjuvant therapy is treatment before the main course of action. Adjuvant therapy is a type of treatment used in combination with initial therapy to inhibit or stop the growth of cancer cells.
The current standard treatment for malignancies of the breast, lungs, colon, pancreas and ovaries is adjuvant therapy. Before surgery or the intended cure for cancers of the head and neck, lung, or anal regions, combined modalities such as chemotherapy and radiation therapy serve to reduce the tumour.8
Treatment cycle
Chemotherapy drugs can be administered:
IV chemotherapy drugs have a 100% absorption rate, which makes them the most common type. Many drugs impact the entire body and circulate through the bloodstream. Thus, they can also target cancer cells that are not picked up during testing and not reached by radiation or surgery (systemic treatment).
The drugs are injected directly into the damaged area of the body (local chemotherapy), as opposed to being administered via the bloodstream. Cytostatics are administered to cancer patients during chemotherapy at predetermined intervals called treatment cycles or treatment schedules. Various factors influence the number of cycles and the intervals between the individual treatments, including:
- The duration of treatment
- The amount of time the body requires to heal
- The length of the drug's effect
The individual's preferences and overall health influence the specifics of a treatment plan with the research findings.8,9
Risks and adverse effects
Common adverse effects associated with chemotherapy are:
- Myelosuppression
- Mucositis
- Nausea and vomiting
- Diarrhoea
- Alopecia
- Fatigue
- Infertility
- Chemotherapy-induced constipation
- Resistance to chemotherapy (primary resistance occurs before drug administration) and secondary resistance (after drug exposure)
- Neurotoxicity
- Infusion reactions
- Immunosuppression increases the risk of infections
Severe drug extravasation resulting in pain, burning, stinging, erythema, abrupt onset oedema, and tissue necrosis are among the complications.8
Comparison
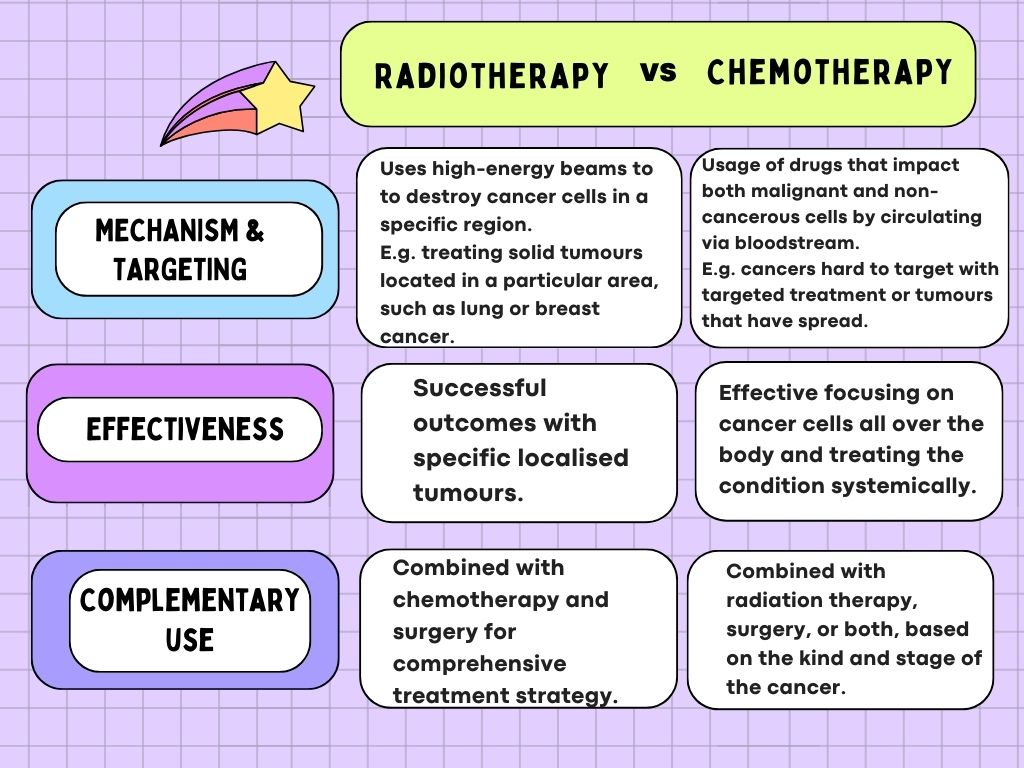
Let's compare and summarise radiation and chemotherapy, as seen in the image below.
Created by: Deepika Rana (Canva)
Treatment planning considerations
Individual participation in cancer treatment decision-making enhances the patient's sense of life quality, physical functioning, patient satisfaction, and quality of care. Making therapy decisions is influenced by the physician's level of expertise. The best decisions are based on high-level evidence by someone knowledgeable about the most recent research and possessing the necessary skills to understand, evaluate, and apply it in a clinical context.13,14
Global cancer control efforts increasingly include early diagnostic initiatives like symptom awareness campaigns. A crucial factor in the timely presentation and evaluation of symptoms is the patients' and physicians' awareness of and assessment of them. Identifying the precise kind and stage of cancer is essential to creating a customised and successful treatment strategy.15
FAQ
What are the techniques for reducing the effects of radiation and chemotherapy on eating?
Reducing nausea and vomiting, preventing a catabolic state and muscle wasting (sarcopenia), and forming therapeutic alliances with patients, carers, and oncologists are some strategies physicians and patients should consider.11
What proportion of cancer cases get treated with radiation therapy?
Approximately 50% of cancer patients undergo radiation therapy at some point during their illness, and it makes up 40% of the curative treatment for the disease.2
What is a significant barrier to effective chemotherapy?
Lack of funds, issues with appointment scheduling (distance to facility, appointment times, long lines, limited appointments), and inadequate or incorrect information about chemotherapy were some of the major obstacles to starting and sticking with chemotherapy.10
Do chemotherapy and radiation treatments have more advanced techniques?
Intensity-modulated radiation treatment (IMRT) and positron emission tomography (PET-CT) are two examples of novel therapy planning and delivery technologies developed in the radiation field. The development of enhanced supportive care agents enables the administration of dose-dense chemotherapy with targeted chemotherapy for treating particular malignancies.12
Summary
The subtle distinctions between chemotherapy and radiation therapy are crucial for developing individualised and successful cancer treatment regimens. While chemotherapy's systemic approach makes it useful for a broader spectrum of tumours, radiotherapy is preferred when treating confined lesions. The tailored strategy, considering the particulars of the cancer diagnosis, guarantees that patients receive the most effective and appropriate interventions, maximising their prospects of success.
References
- Abbas Z, Rehman S. An overview of cancer treatment modalities. In: Neoplasm [Internet]. IntechOpen; 2018 [cited 2023 Dec 11]. Available from: https://www.intechopen.com/chapters/60895
- Baskar R, Lee KA, Yeo R, Yeoh KW. Cancer and radiation therapy: current advances and future directions. Int J Med Sci [Internet]. 2012 Feb 27 [cited 2023 Dec 11];9(3):193–9. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3298009/
- Krzyszczyk P, Acevedo A, Davidoff EJ, Timmins LM, Marrero-Berrios I, Patel M, et al. The growing role of precision and personalised medicine for cancer treatment. Technology (Singap World Sci) [Internet]. 2018 [cited 2023 Dec 11];6(3–4):79–100. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6352312/
- Maani EV, Maani CV. Radiation therapy. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Dec 11]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK537036/
- Burnet NG, Thomas SJ, Burton KE, Jefferies SJ. Defining the tumour and target volumes for radiotherapy. Cancer Imaging [Internet]. 2004 Oct 21 [cited 2023 Dec 11];4(2):153–61. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1434601/
- Chaput G, Regnier L. Radiotherapy. Can Fam Physician [Internet]. 2021 Oct [cited 2023 Dec 12];67(10):753–7. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8516179/
- Sugerman, MSW DT. Chemotherapy | Oncology | JAMA | JAMA Network [Internet]. JAMA Network | Home of JAMA and the Specialty Journals of the American Medical Association. JAMA Network; 2013 [cited 2023 Dec 12]. Available from: https://jamanetwork.com/journals/jama/fullarticle/1710460
- Amjad MT, Chidharla A, Kasi A. Cancer chemotherapy. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Dec 13]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK564367/
- How does chemotherapy work? In: InformedHealth.org [Internet] [Internet]. Institute for Quality and Efficiency in Health Care (IQWiG); 2019 [cited 2023 Dec 13]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279427/
- McMahon DE, Singh R, Chemtai L, Semeere A, Byakwaga H, Grant M, et al. Barriers and facilitators to chemotherapy initiation and adherence for patients with HIV-associated Kaposi’s sarcoma in Kenya: a qualitative study. Infect Agent Cancer [Internet]. 2022 Jul 6 [cited 2023 Dec 13];17:37. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9258164/
- Anderson PM, Thomas SM, Sartoski S, Scott JG, Sobilo K, Bewley S, et al. Strategies to mitigate chemotherapy and radiation toxicities that affect eating. Nutrients [Internet]. 2021 Dec 8 [cited 2023 Dec 13];13(12):4397. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8706251/
- Heron DE, Shogan JE, Mucenski JW. Innovations in chemotherapy and radiation therapy: Implications and opportunities for the Asia-Pacific Rim. Biomedical Imaging and Intervention Journal [Internet]. 2008 Sep [cited 2023 Dec 13];4(3). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3097728/
- Noteboom EA, May AM, van der Wall E, de Wit NJ, Helsper CW. Patients preferred and perceived level of involvement in decision making for cancer treatment: A systematic review. Psychooncology [Internet]. 2021 Oct [cited 2023 Dec 13];30(10):1663–79. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8518833/
- Glatzer M, Panje CM, Sirén C, Cihoric N, Putora PM. Decision-making criteria in oncology. Oncology [Internet]. 2018 Sep 18 [cited 2023 Dec 13];98(6):370–8. Available from: https://doi.org/10.1159/000492272
- Koo MM, Swann R, McPhail S, Abel GA, Elliss-Brookes L, Rubin GP, et al. Presenting symptoms of cancer and stage at diagnosis: evidence from a cross-sectional, population-based study. Lancet Oncol [Internet]. 2020 Jan [cited 2023 Dec 13];21(1):73–9. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6941215/




