

Introduction
Lipodystrophy is derived from 2 Latin words – “Lipo” which means fat, and “dystrophy”, which means derangement. Put together, lipodystrophies are a group of conditions characterised by the loss and/or derangement of fatty tissues in the body. These conditions are grouped into 2 main categories: inherited and acquired.1
Inherited lipodystrophies are also called genetic lipodystrophies, and they are caused by an inherited defect gene or group of genes. Acquired lipodystrophies (AL) are not inherited and usually occur later in life. In this article, we will be focusing on the group of acquired lipodystrophies.2
Lipodystrophies are a very rare group of conditions, although the acquired lipodystrophies are more common than the inherited lipodystrophies. It is estimated that 200 people in the UK have lipodystrophy, and for the general populace, it is an average of 2 in a million people.3
Types of acquired lipodystrophy
There are 2 major types of acquired lipodystrophy (AL), and they are Acquired Partial Lipodystrophy (APL) and Acquired Generalized Lipodystrophy (AGL). Of these 2 groups, APL is more common and less severe.4
Acquired partial lipodystrophy (APL)
APL is also known as Barraquer-Simons Syndrome, and it is a special type of lipodystrophy in which there is a loss of subcutaneous body fat that typically progresses from the head down. This type usually doesn’t affect the legs. It is more common in Europeans and 4-8 times more common in people assigned female at birth (people AFAB) than in people assigned male at birth (people AFAB). It usually occurs in adolescents but can be seen in people above the age of 40 years.1,5,6
APL is the most common type of Lipodystrophy, especially since HIV-associated APL has been discovered. There are other conditions associated with APL, and they will be discussed in this article. Currently, over 100,000 cases of APL have been recorded, with the majority of the cases being HIV-related. 4
In HIV-related APL, there is subcutaneous fat loss in the face, arms, and legs in people with HIV taking treatment- Highly active antiretroviral therapy (HAART). APL doesn’t usually affect the legs, but this happens in people taking HAART. Sometimes, there is fat deposition in the abdomen and back of the neck, creating what is called a buffalo hump. Other times, you have both fat loss and fat deposition. It is not known why people receiving this treatment have this condition, but it is purported that some of the medications used could cause some destruction of fat cells in the body.4,1
Another possible condition related to APL is the reduction of a particular substance in the body called complement 3 (C3) and the increased levels of another substance called C3 nephritic factor. The combination of these 2 substances leads to fat cell destruction. The exact reason why it destroys the fat cells mostly in the head, neck, arms, chest, abdomen, and not legs is unknown. In some cases, it does affect all the subcutaneous fat cells in the body and causes generalized lipodystrophy. The substance C3 nephritic factor also increases the likelihood of those who have this kind of APL to have kidney diseases.1,4,6
Bone marrow transplant has also been related to APL. This type of APL shows subcutaneous fat loss in the head, arms, and buttocks. In bone marrow transplant, the recipient must take very strong medications and sometimes get exposed to radiation to make sure that their body can accept the bone marrow being given to them. Even with that, some might get reactions caused by their bodies fighting the bone marrow given to them because they perceive it as foreign. Some experts purport that the preparation patients must undergo for this procedure (Bone marrow transplant) and the reactions that can occur after the procedure could cause the destruction of body fat, leading to APL.1
Acquired generalized lipodystrophy (AGL)
Acquired Generalized Lipodystrophy, also called Lawrence syndrome, is less common than APL. Only about 85 cases have been reported worldwide. In this condition, there is subcutaneous fat loss all over the body. The only exception is the fat behind the eyes and the fat in the bone marrow. Women are more likely to have this condition, three times more than men, and it affects Caucasian women more.1,4,5
Fat loss isn’t noticed at birth, so children appear normal but begin to develop the appearance as they grow older. Some conditions have been linked to AGL, but 50% of all cases of AGL have no known or suspected cause.6
One of the conditions related to AGL is called Panniculitis. It has been noted that about 25% of people with AGL also have this disease called Panniculitis and it was likely the triggering factor for APL. The fat loss seen in this type of AGL starts patchy from the injuries caused by panniculitis and then progresses into complete fat loss all over the body.1,4,6
Autoimmune conditions have also been associated with AGL. About 25% of AGL patients have some form of autoimmune disease, the most common being juvenile dermatomyositis. The average age of patients seen with this type of AGL is 15 years.1,4
Acquired localized lipodystrophy (ALL)
There is another class of acquired lipodystrophy, and it is called ALL. In this class, fat loss affects smaller areas of the body where some injuries may have occurred or medications were given. It is usually not related to any conditions.1,4
Pathogenesis of acquired lipodystrophy
Pathogenesis simply means the progression of a disease. In this section, we will be talking about the various causes(suspected) of AL and how the disease develops.
Lipodystrophy is closely related to Obesity even though it is so strikingly different. Their similarities are seen in the way the disease develops. In AL (and inherited lipodystrophy as well), there is a problem with the safe storage of fat in the body. Fat cannot be safely stored under the skin(subcutaneous) because of the destruction of the subcutaneous fat tissues in AL. Fat is then deposited in unsafe places, such as around/in our organs and in our blood vessels. This leads to all kinds of diseases, such as hypertension, Diabetes Mellitus, and other severe and chronic conditions.1
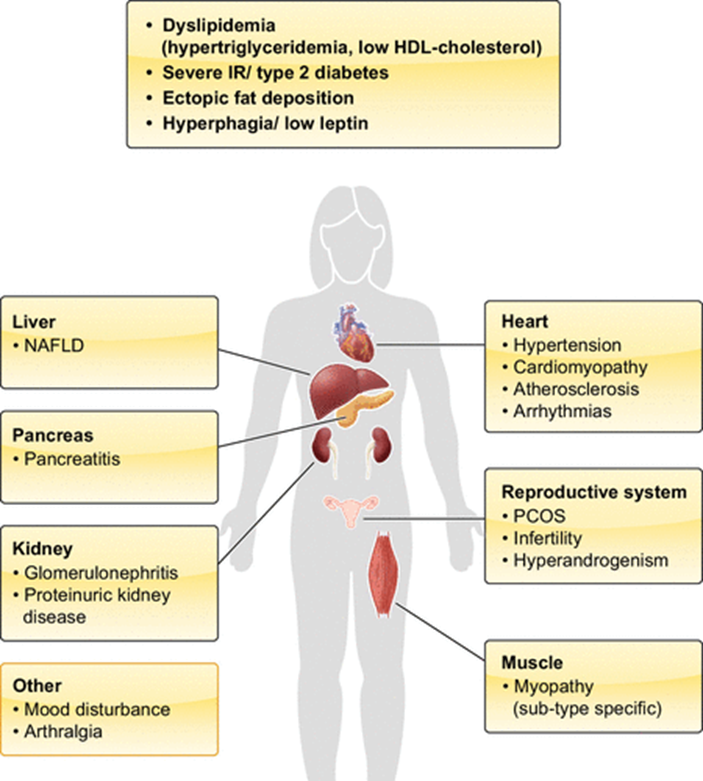
Fig.1- Key tissues/organs commonly affected in lipodystrophies.1
Also, fatty tissues produce a particular substance called leptin that regulates feeding and lets you know when you’re full. A loss of fatty tissues means reduced amounts of this substance, causing those who have AL (and inherited Lipodystrophy) to have insatiable appetites which lead to more unsafe fat deposition, and the cycle goes on. People with AL appear slim and toned but have all the diseases associated with obesity.1
Clinical presentation
Acquired lipodystrophy can appear different for each of the subtypes we talked about. This is because of the varied likely causes and how they affect the body. We would divide the features of this disease into Physical and Metabolic to better understand how AL appears.
Physical features
The major physical change is the loss of subcutaneous fat. Because of this, a person with AL may appear toned with defined muscles and veins. In AGL, this look affects the entire body, including the breasts in females, but in APL, it usually affects the upper part of the body, excluding the legs.
Sometimes, especially in HIV-associated APL, the fat loss affects the legs and spares the abdomen. There is also extra deposition of fat in the neck, chin, and back causing a double chin and buffalo hump appearance.
In the other APL subtypes, there is an increase in fat deposition in the legs and hips as though compensating for the loss of fat in the upper body.
People with APL usually have a voracious appetite because of how the disease works.
There may also be signs of other diseases associated with APL. For instance, vitiligo is a condition associated with APL, and the features of patches of pale skin may be seen in people with APL. 1,4,5,6
Metabolic features
The metabolic abnormalities vary in severity from APL to AGL, with APL having less severe changes than AGL. ALL isn’t associated with any metabolic changes as the cause is usually almost external (medications, injuries, and so on).
Some of the metabolic abnormalities seen in AL include insulin resistance and abnormal cholesterol, and their resultant effects are seen in the picture above.1,4,5,6
Diagnosis and evaluation
Usually, a medical practitioner can tell if a patient has acquired lipodystrophy by the symptoms they have and their physical features, but several tests can be done to check how much AL has affected organs in the body. For instance, scans can be done to check the level of damage to the liver, the kidneys, or the ovaries. Blood tests can be done to check the levels of cholesterol and sugar in the blood. Special scans of the muscles can be done to show abnormal muscular growth.2,5
Treatment and prognosis
Although there have been several experiments working towards a cure for AL, no known treatment has been found that can reverse the course of the condition. This disease is currently managed by treating its effects on the body.
It is generally accepted that eating healthy and adequate meals is a good first step. People who have AL tend to always feel hungry, and overeating just worsens the condition. Monitoring the amount of food you eat, and eating healthy, low-fat meals can help slow the progression of the disease.1
Exercise may also benefit patients with AL. This might be difficult to do because of the muscle aches that are seen in this condition. Also, women may feel they already look too masculine and may not want to do any additional exercise, but keeping active can help reduce the disease progression.1
Other conditions caused by this disease, such as Diabetes, Hypertension, High Blood Cholesterol, and PCOS, are treated just as they would be treated in a patient without AL.1,4,6
A particular medication that mimics the leptin hormone has been manufactured but is used only rarely to treat people with AL. This medication is called metreleptin and is only used in conjunction with other measures like exercise and healthy eating.3
Some medical practitioners have considered cosmetic surgeries to improve the facial appearance of those with AL, especially HIV-associated APL.4
Because this disease can cause adverse emotional and psychological effects, the involvement of therapists, social groups, possible medications (such as antidepressants), and especially family support is very important in its management. It is important to go to a health facility if you feel you have this condition so that you can be properly examined and given prompt management. The health facility would also be the best place to find social groups that would cater to you.
Conclusion
Acquired lipodystrophy is a disorder that has to do with the loss and/or derangement of fatty tissues in the body. Although it is quite rare, it is a source of immense concern for those who suffer from the condition and their loved ones. It is very difficult to manage currently with treatment involving a wide range of specialities due to the complications of this disease. However, there is hope for better management because a lot of research is ongoing, and who knows, a permanent cure might be found for this rare, devastating disease.
References
- Lim, Koini, et al. ‘Lipodystrophy: A Paradigm for Understanding the Consequences of “Overloading” Adipose Tissue’. Physiological Reviews, Dec. 2020, p. physrev.00032.2020. DOI.org (Crossref), https://doi.org/10.1152/physrev.00032.2020.
- Zammouri, Jamila, et al. ‘Molecular and Cellular Bases of Lipodystrophy Syndromes’. Frontiers in Endocrinology, vol. 12, 2022. Frontiers, https://www.frontiersin.org/articles/10.3389/fendo.2021.803189.
- The Condition | Metreleptin for Treating Lipodystrophy | Guidance | NICE. 24 Feb. 2021, https://www.nice.org.uk/guidance/hst14/chapter/2-The-condition.
- Garg, Abhimanyu. ‘Acquired and Inherited Lipodystrophies’. New England Journal of Medicine, vol. 350, no. 12, Mar. 2004, pp. 1220–34. DOI.org (Crossref), https://doi.org/10.1056/NEJMra025261.
- Quinn, Kelly, et al. ‘Lipodystrophies’. StatPearls, StatPearls Publishing, 2023. PubMed, http://www.ncbi.nlm.nih.gov/books/NBK459180/.
- Fiorenza, Christina G., et al. ‘Lipodystrophy: Pathophysiology and Advances in Treatment’. Nature Reviews. Endocrinology, vol. 7, no. 3, Mar. 2011, pp. 137–50. PubMed Central, https://doi.org/10.1038/nrendo.2010.199.




