


Introduction
Acrophobia, often referred to as the fear of heights, is a complex and diagnosable psychological condition that goes beyond mere discomfort at the sight of heights. It involves an intense and irrational fear of falling, often despite the absence of real danger. Around 3-6% of the population suffer from acrophobia, and it can be distinguished from the less severe condition known as visual height intolerance, which is present in around 30% of the population.1
Addressing acrophobia is essential, as its impact can cause significant distress and make some tasks that are trivial or fun for non-sufferers impossible, thereby reducing the overall quality of life of the sufferer. However, it can be very challenging to overcome, and rationality alone is not sufficient for success in this task. Treatment is required to manage and conquer acrophobia effectively.
Symptoms and effects of acrophobia
Individuals suffering from acrophobia often experience an array of physical, emotional, and cognitive manifestations when confronted with heights. Typical first-hand accounts from interviews mention that the sufferer's body is ‘freezing up’ as if there is some kind of mental or physical ‘block’ preventing them from moving. Meanwhile, they are simultaneously overwhelmed by a range of distressing thoughts and emotions. Here is a typical example from a transcribed interview of an acrophobic describing the experience while hiking:1
“I simply couldn’t go any further. It’s like a mental block – I have to sit down, I’m overwhelmed by fear, my heartbeat begins racing so fast that I also feel like I’m suffocating, I can’t breathe anymore…”
However, the experience of acrophobia is highly individual, and it may be experienced differently from the way described above.
Physical symptoms
- Heart palpitations
- Unsteadiness
- Sweating
- Trembling
- Weakness in the knees
- Drowsiness
- Nausea
Emotional and cognitive symptoms
- Anxiety
- Fearfulness
- Panic attacks
- Dizziness and vertigo
- Agitation
- Avoidance behaviour
Impact on daily life
The impact of acrophobia on daily life can be quite significant. It can interfere with work, making tasks that involve encountering heights challenging or impossible.
Travel, particularly air travel or travel involving bridges, becomes a daunting prospect and is thus often avoided. Even leisure activities such as hiking, climbing, or enjoying scenic viewpoints are curtailed by fear, thereby degrading the overall quality of life.
Understanding acrophobia
What happens during a height-related anxiety and fear?
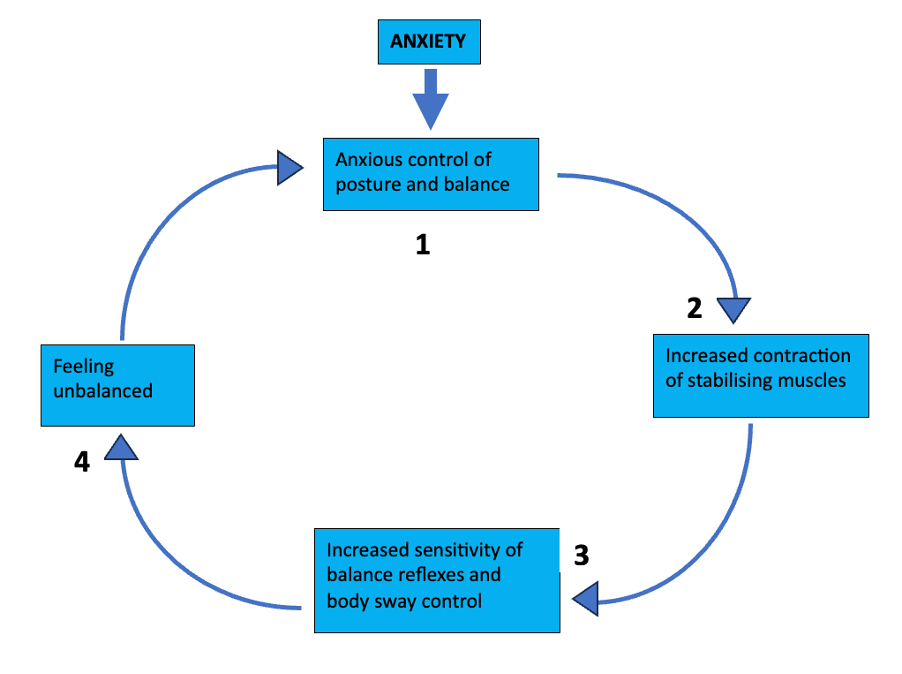
When standing on elevated surfaces, the body undergoes postural changes to counter the perceived threat. Various stabilising muscles tense, resulting in stiffening, and balance reflexes become more sensitive. These changes result in gait changes such as slower walking speed, shorter steps, irregular rhythm, and a longer period of time where both feet are on the ground.2
However, in acrophobic and at-risk individuals, these changes are significantly more pronounced. These individuals are also seen to have significantly more body sway, perform poorly on balance-related tasks, and have limitations of head and eye movements in certain directions.3 Essentially, acrophobic individuals are almost ‘scared stiff’, with an overactivation of the musculoskeletal and nervous system and a frozen gaze fixed on the horizon. All of these changes, particularly the freezing of gaze, may actually disrupt their ability to properly sense their balance and cause the feeling of instability, and the resulting anxiety that follows.1
Various experiments have indicated that this cautious way of walking and the restriction of visual exploration is driven by fear and anxiety rather than the perception of real, absolute height itself.4,5 The higher the level of anxiety, the more pronounced these postural and visual changes are.6
These findings, taken together, can lead to a conceptualisation of a cascade of events, resembling a vicious cycle which can account for the symptoms experienced in acrophobia, as shown in the figure below:
Causes and triggers of acrophobia
Acrophobia often arises from non-associative learning rather than trauma-induced conditioning. That is to say, to develop acrophobia, you don’t need to have experienced a negative event related to height, it usually develops spontaneously. However, susceptibility to acrophobia may be influenced by personality traits and genetics. It usually starts in childhood or early adulthood and it tends to stay constant rather than fluctuating, persisting for decades if left untreated.1
Once acrophobic, the symptoms can be triggered by a range of height-related scenarios. The most common are:
- Climbing a tower
- Hiking
- Climbing a ladder
- Walking over a bridge
- Working on the roof of a building
- Sitting on a Ferris wheel7
Increasing the height level tends to heighten anxiety in acrophobic individuals. They also react more strongly to height increases than non-acrophobics. However, beyond approximately 70 metres, the anxiety level seems to plateau in most acrophobic cases. In non-acrophobic cases, this plateau occurs at around 40 metres.1
Relationship between acrophobia and evolutionary psychology
Evolutionary psychology offers insights into the root of acrophobia in the fight/flight/freeze response. Our body systems, such as visual and vestibular systems, have been refined by the process of evolution through natural selection to perform specific functions that are suited to our environment. However, body systems are not well suited for certain scenarios, particularly those in which they must work together in an integrated manner. Sometimes, a significant and imminent threat may be perceived when there isn’t one. Moving on a horizontal plane at a great height is one of those situations, as both of these systems, visual and vestibular, are doing the job they have been refined to perform, but they both receive conflicting information which cannot be reconciled,8 generating a feeling of instability despite the plane being stable. In susceptible individuals, this feeling of instability is especially pronounced and activates fear responses and anxiety.
It is thought the anxiety-induced stiffening, increased sensitivity of balance reflexes, and rigid body sway regulation in such individuals may be the activation of the primitive “feigning death” reflex mechanism, which originally evolved to increase chances of survival.1
Diagnosis and Differentiation
Acrophobia falls under ‘specific phobias’ in the literature of two main methods of classifying and characterising illnesses globally: the International Classification of Diseases, 10th Revision ICD-10 and The Diagnostic and Statistical Manual of Mental Illnesses (DSM-5).9
Distinguishing acrophobia from ‘healthy caution’
Most people find it hard to stay steady when they are at a significant height. This is because stationary objects located on the ground are far away, and it is, therefore, tough for your eyes to guide your body in the right way to maintain balance. This is a normal response and not a cause for concern.
However, some individuals are particularly susceptible to anxiety arising from this subjective instability and may experience the cascade of events shown in the diagram above. In fact, around 30% of people experience distress and anxiety when exposed to heights, but this is below the threshold for a diagnosis of a specific phobia according to ICD-10 or DSM5 and so, instead, they fall into the separate category of ‘Visual Height Intolerance’ used in the scientific literature. Around 50% of these individuals may still require treatment to overcome the symptoms.1
People may be diagnosed with acrophobia by a medical professional when symptoms are severe enough to significantly impact the quality of life and lead to avoidance of triggers wherever possible. The ICD-10 would be used in the UK as a guideline for assisting diagnosis. This states that for a diagnosis of acrophobia, there must be intense fear, avoidance of exposure to heights, at least one of the ‘vegetative’ symptoms such as trembling, sweating, palpitation, and two other symptoms from their symptoms list.9
Additionally, tools like the Heights Interpretation Questionnaire help in gauging the severity of fear and are often used in research, but are not officially recommended in the clinical situation.10
Co-occurring conditions
Acrophobia frequently co-occurs with anxiety (16.75%) and depressive disorders (26.1%). It Is also highly prevalent in various vestibular diseases, including vestibular migraine (61%) and phobic postural vertigo (64%). Furthermore, approximately 30% of individuals use medication or alcohol to manage acrophobia-related anxiety.
Overcoming acrophobia
In acrophobic individuals, there is variation in the course of illness. In one study, only around 23% were found to have improved or completely resolved symptoms, whereas the remaining 77% had persistent or worse symptoms. They also found that the presence of other conditions worsened the course of the condition, such as depression, other phobias, post-traumatic stress disorder (PTSD), and a traumatic original source of the acrophobia.11
In the cases where remission occurred, it often took months or years to achieve. This may be due to a variety of reasons. For one, despite the proven efficacy of various therapies in treating specific phobias, a very low proportion of phobia-susceptible individuals seek medical treatment, especially for fear of heights. Furthermore, for those who sought treatment for their fear of heights, there is a history of poor treatment advice, including medication and unspecific behavioural advice. Consequently, it was found that only one-third of individuals seeking help received an improvement in symptoms.11 However, this may now be improving due to a better understanding of the condition.
Guided exposure therapy
In a similar manner to many other phobias, gradual exposure to heights combined with breathing exercises and mindfulness can desensitise individuals to fear. Whereas, avoiding all triggering situations can maintain sensitisation and promote the persistence of the condition.12
It is recommended that a medical professional is consulted for exposure therapy treatment. They can provide evidence-based, effective, and safe therapy, monitoring progress to ensure the phobia is overcome efficiently and in a safe and healthy way. In some instances, medications like antidepressants and anxiolytics may be prescribed as these can manage the fear and anxiety symptoms, allowing the individual to engage in exposure therapy more effectively.
Recent research on the mechanisms behind the fear of heights has illuminated some specific behaviours you can use when encountering heights to counter each visual, vestibular, and cognitive system change that occurs.1 If recommended by a medical professional, to counteract visual effects, you could:
- Fix your eyes on the horizon
- Look at near stationary objects or at least aim to keep them in the peripheral vision
- Avoid looking at large, slowly moving objects in the distance, such as clouds.
- Don’t look through binoculars without a stabilising support, e.g, a railing.
- Close your eyes when standing
For effects arising from body position and movement, you could:
- Stop walking
- Sit or lie down
- Lean or hold tight onto something
For cognitive effects, you could:
- Focus on overcoming avoidance
- Perform a simple but distracting task, such as naming items in a category.
FAQs
Are there different degrees of acrophobia?
Yes, the severity of acrophobia, the severity with which the accompanying symptoms present, and also the sensitivity to height increases can vary between acrophobic individuals. Some individuals may feel anxious at certain heights, while others might experience disabling panic attacks, vertigo, and nausea at any height above 3 metres.
Is acrophobia the same as vertigo?
No, acrophobia is not the same as vertigo. Acrophobia is a fear of heights, whereas vertigo is a specific type of dizziness or sensation of spinning.
Can acrophobia develop suddenly?
Acrophobia can develop suddenly after a traumatic experience involving heights, spontaneously, or gradually over time due to learned behaviours or negative experiences.
Summary and conclusion
Acrophobia, commonly known as the fear of heights, is a distinct psychological condition characterised by an intense and irrational fear of falling, even when there's no real danger. Around 3-6% of the population have acrophobia, which differs from the milder condition of visual height intolerance, which affects about 30% of people, and general caution around heights, which affects nearly everyone. Overcoming acrophobia is crucial, given its potential to cause significant distress and to curtail or impair daily activities that involve heights.
People with acrophobia often experience a range of physical, emotional, and cognitive symptoms when confronted with heights. These symptoms may include a sensation of "freezing up," rapid heartbeat, suffocation-like feelings, and overwhelming fear, which are a result of an overreaction of postural and visual system changes that initially evolved to keep us safe.
Acrophobia can severely impact daily life, making tasks like work, travel, and leisure activities challenging or even impossible. It also co-occurs with other psychiatric and neurological disorders. Therefore, it is essential to see a medical professional for diagnosis and appropriate treatment. Research has indicated several behavioural techniques that can be of use during treatment.
References
- Huppert D, Wuehr M, Brandt T. Acrophobia and visual height intolerance: advances in epidemiology and mechanisms. J Neurol. 2020; 267(Suppl 1):231–40.
- Wuehr M, Kugler G, Schniepp R, Eckl M, Pradhan C, Jahn K, et al. Balance control and anti‐gravity muscle activity during the experience of fear at heights. Physiol Rep [Internet]. 2014 [cited 2023 Nov 26]; 2(2):e00232. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3966255/.
- Kugler G, Huppert D, Eckl M, Schneider E, Brandt T. Visual Exploration during Locomotion Limited by Fear of Heights. PLoS One [Internet]. 2014 [cited 2023 Nov 26]; 9(8):e105906. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4148313/.
- Brown LA, Gage WH, Polych MA, Sleik RJ, Winder TR. Central set influences on gait. Age-dependent effects of postural threat. Exp Brain Res. 2002; 145(3):286–96.
- Tersteeg MCA, Marple-Horvat DE, Loram ID. Cautious gait in relation to knowledge and vision of height: is altered visual information the dominant influence? J Neurophysiol. 2012; 107(10):2686–91.
- Donnelly MR, Reinberg R, Ito KL, Saldana D, Neureither M, Schmiesing A, et al. Virtual Reality for the Treatment of Anxiety Disorders: A Scoping Review. Am J Occup Ther [Internet]. 2021 [cited 2023 Nov 26]; 75(6):7506205040. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8742249/.
- TEGGI R, COMACCHIO F, FORNASARI F, MIRA E. Height intolerance between physiological mechanisms and psychological distress: a review of literature and our experience. Acta Otorhinolaryngol Ital [Internet]. 2019 [cited 2023 Nov 26]; 39(4):263–8. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6734202/.
- ICD-10-CM - 2024 Tabular List of Diseases. ICD-10 Coded [Internet]. [cited 2023 Nov 26]. Available from: https://icd10coded.com/cm/.
- Steinman SA, Teachman BA. Cognitive processing and acrophobia: validating the Heights Interpretation Questionnaire. J Anxiety Disord. 2011; 25(7):896–902.
- Kapfhammer H-P, Fitz W, Huppert D, Grill E, Brandt T. Visual height intolerance and acrophobia: distressing partners for life. J Neurol [Internet]. 2016 [cited 2023 Nov 26]; 263(10):1946–53. Available from: http://link.springer.com/10.1007/s00415-016-8218-9.
- Thomas Brandt DH. Fear of Heights and Visual Height Intolerance in Children 8â10 Years Old. J Child Adolesc Behav [Internet]. 2015 [cited 2023 Nov 26]; 03(04). Available from: http://www.esciencecentral.org/journals/fear-of-heights-and-visual-height-intolerance-in-children-810-years-old-2375-4494-1000219.php?aid=58662




