


Introduction
Chilaiditi’s syndrome, named after the radiologist Demetrius Chilaiditi, is a rare condition characterised by the presence of a section of the gut in between the liver and the diaphragm. Most times, this does not cause symptoms, but when it does, it is called Chilaiditi syndrome.
Chilaiditi’s syndrome is a very rare syndrome seen in less than 0.5% of the entire population. It affects individuals assigned males at birth four times more frequently than individuals assigned females at birth and is seen more commonly in the elderly than in the younger population. It is an important syndrome because it is often misdiagnosed for a surgical emergency called pneumoperitoneum, in which gas or air fills the space surrounding the abdominal organs.1
How does chilaiditi’s syndrome occur?
To understand Chilaiditi’s syndrome, we must first understand the locations of the different organs in the abdomen. In particular, pay attention to the position of the liver, diaphragm, and bowels, as they are the ones involved in this rare syndrome. Below is a pictorial representation of these intra-abdominal organs.
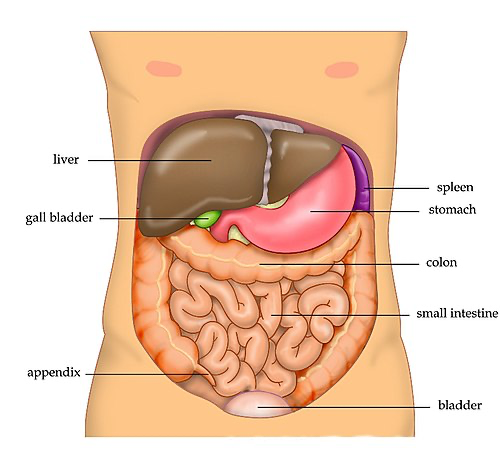
Photo from Wikipedia (https://en.wikipedia.org/wiki/Abdomen)
The diaphragm lines the top of the abdomen and extends from the right to the left side of the abdomen. The liver is a large organ located just below the diaphragm and mostly in the top right quadrant (quarter) of the abdomen. The colon is the part of the gut situated just below the liver, encircling the small intestine. The colon is divided into 3 sections, known as the ascending, transverse, and descending colon.
In Chilaiditi’s syndrome, a part of the colon (or rarely, the small intestine) is interposed between the liver and the diaphragm.2 This usually happens sporadically and can be caused by structural abnormalities you were born with. However, Chilaiditi’s syndrome can also be caused by some medical conditions, which will be discussed in the next section.2
What causes chilaiditi’s syndrome?
Because Chilaiditi’s syndrome is so rare, not much is known about what causes it. However, most researchers believe that Chiliaditi’s syndrome can be divided into two groups: congenital (present at birth) and acquired (develops during life).2
Congenital Chilaiditi's
Congenital Chilaiditi is usually caused by defects or variations in the body’s anatomy that are present from childbirth. Usually, the colon is held in place by fibrous tissues known as ligaments. Sometimes, these ligaments are lax or absent and, therefore, do not hold the colon in place and increase the likelihood of the colon getting interposed between the diaphragm and the liver. Other defects, such as the malposition of the organs in the abdomen, can also make it possible for Chilaiditi’s syndrome to occur in an individual.
Acquired chilaiditi's
Acquired causes are not present at birth but instead develop due to illnesses or some lifestyle factors. Possible causes of acquired Chilaiditi’s syndrome include:
- The colon is larger than usual. This can be caused by toxic megacolon and is commonly seen in specific bowel disorders like ulcerative colitis. Aerophagia is another cause of a large colon. It is an abnormal gas accumulation in the colon due to the excessive swallowing of air. Any of these conditions could increase the chance of a part of the colon getting in between the liver and the diaphragm.
- Paralysis of the nerve supplying the diaphragm. This leads to the diaphragm becoming raised, leaving enough space between the diaphragm and the liver for the colon to get stuck in.
- Some chest conditions, such as chronic COPD, increase your chance of Chilaiditi’s syndrome.
- Cirrhosis is a condition that causes the liver to shrink and has been implicated in Chilaiditi’s syndrome.
- Any condition that increases the pressure in the abdomen (ascites, obesity, or multiple pregnancies) may cause Chilaiditi’s syndrome.
- Certain medical interventions, like psychotropic medications, have been known to trigger the interposition of the colon between the liver and the diaphragm.1-3
- Other medical procedures have also been noted to cause Chilaiditi’s syndrome in some individuals. These procedures include colonoscopy, bariatric surgery or the insertion of a feeding tube.3
Symptoms of chilaiditi’s syndrome
Chilaiditi’s syndrome often does not cause any symptoms. In these cases, it is found purely by chance. In other cases, however, Chilaiditi’s can cause abdominal pain, nausea, constipation, and vomiting. Less commonly reported symptoms include chest pain, difficulty in breathing and an abnormal heart rhythm.4 These symptoms may worsen when you lay down.3
Chilaiditi’s syndrome occasionally causes life-threatening complications that require immediate attention. The part of the bowels stuck in between the liver and the diaphragm can become twisted, causing an intestinal obstruction. This causes severe abdominal pain, complete constipation, and vomiting. If that obstruction is not relieved, it can cause holes to form in the bowels (known as “perforated bowel”). This is a very serious complication that can quickly lead to death if not acted upon immediately.1,4
Diagnosis
Chilaiditi’s syndrome is diagnosed by using radiological investigations such as CT scans and X-rays. There are no symptoms specific to this syndrome, so it is often difficult to investigate and diagnose. Further complicating matters is that Chilaiditi’s syndrome can mimic different medical conditions, so an accurate and confident diagnosis will require a thorough investigation. Several conditions must be met to confirm a diagnosis of Chilaiditi’s syndrome:
- The right hemidiaphragm must be raised.
- The misplaced bowel must be distended with air
- The liver must be positioned lower than the left side of the diaphragm
On a plain X-ray, Chilaiditi’s syndrome will appear as a dark shadow under the right side of the diaphragm. The dark shadow represents the air in the section of the colon between the liver and the diaphragm. The bowels have a distinctive appearance on the plain x-ray and look somewhat like tubes with special markings within them. These markings are called haustra markings and are what distinguishes Chilaiditi’s syndrome from the surgical emergency pneumoperitoneum. In the pneumoperitoneum, there is also a dark shadow underneath the diaphragm, but no markings are seen. These markings help us diagnose Chilaiditi’s syndrome. However, a better way to diagnose this syndrome is by doing a CT scan. A CT scan is much clearer and shows the bowels better than an X-ray.
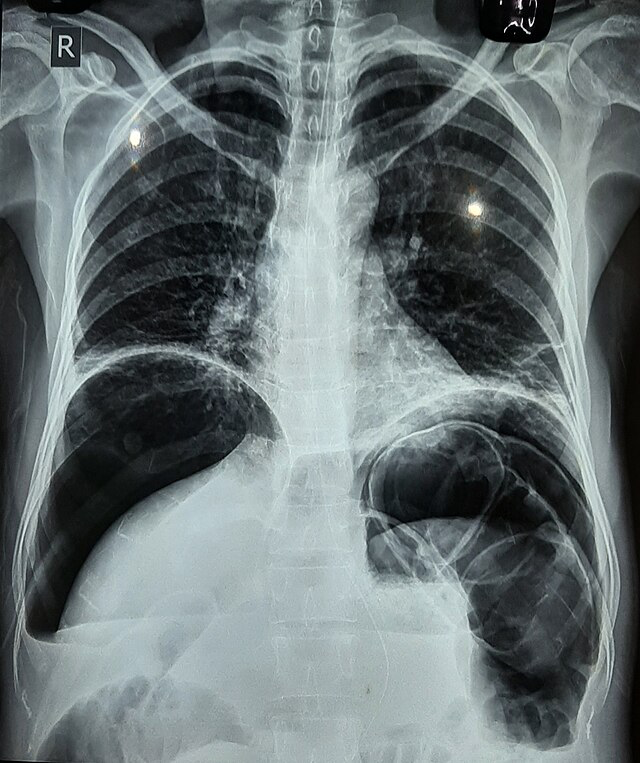
X-ray showing Chilaiditi’s sign. Image from Wikimedia Commons (https://upload.wikimedia.org/wikipedia/commons/thumb/2/2f/Chilaiditi_Syndrome.jpg/640px-Chilaiditi_Syndrome.jpg)
After diagnosing this syndrome, more questions, examinations, and tests may be done to find its most likely cause. A shrunken liver can be seen on an ultrasound scan, and the conditions associated with it can be diagnosed by asking specific questions and running some more tests. The same goes for other possible causes of Chilaiditi’s syndrome.1,4
Treatment and management
No treatment is required for asymptomatic Chilaiditi’s syndrome. Instead, medical professionals will observe the patient and watch them closely in case they develop symptoms later on.
In symptomatic cases of Chilaiditi’s syndrome, initial management aims to decompress the abdomen and provide fluids. You should also stay in bed to rest. The abdomen is decompressed using laxatives, enemas, and a nasogastric tube, which is passed through the nose into the stomach to help drain and decompress it. Fluids are usually given through an IV, and the bowels are rested. In most cases, the symptoms and internal disruption seen on an X-ray or CT scan resolve quickly.
Symptomatic cases that do not respond to this initial management are treated using various surgical procedures, with the procedure(s) chosen depending on the ongoing complication.1,2,3,4
Prognosis
Chilaiditi syndrome usually causes no symptoms. When it does, it spontaneously resolves most of the time. However, if you are found to have Chilaiditi’s syndrome, there is a high probability you will experience bouts of the syndrome throughout your lifetime. Rarely, Chilaiditi’s syndrome can cause severe complications, which, if left untreated, can be fatal.
Summary
Whilst Chilaiditi’s syndrome is often harmless, it is very important to understand its symptoms due to its similarities to serious medical conditions. The radiological features of Chilaiditi’s syndrome are very similar to those seen in the surgical emergency room, called pneumoperitoneum, and can sometimes mask the presence of an ongoing pneumoperitoneum. It is vital to be aware of this syndrome as a misdiagnosis could either lead to a delay in surgical interventions or lead to an unrequired surgery.
References
- Weng W, Liu D, Feng C, Que R. Colonic Interposition between the Liver and Left Diaphragm - Management of Chilaiditi Syndrome: A Case Report and Literature Review. Oncol. Lett. 2014;7:1657-1660.
- Kapania EM, Link C, Eberhardt JM. Chilaiditi Syndrome: A Case Report Highlighting the Intermittent Nature of the Disease. Case Reports in Medicine. 2018;2018:3515370.
- Kumar A, Dhruv M. Chilaiditi Syndrome. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Jan 2024. Available at: http://www.ncbi.nlm.nih.gov/books/NBK554565/.
- Tariq HA, Tharuneshan P. The Air up There - Chilaiditi’s Syndrome: A Case Report and Review of the Literature. Afr. J. Emerg. Med. 2020;10:266-268.
- Moaven O, Hodin RA. Chilaiditi Syndrome. Gastroenterol. Hepatol. 2012;8:276-278.
- Dsouza S, Mhaske Y, Kulkarni A, Baviskar A.Chilaiditi Syndrome—a Clinical Conundrum! South. Afr. J. Anaesth. Analg. 2018; 24:170-171.




