

Introduction
The medical condition known as coccydynia is characterised by pain and discomfort in the coccyx. It’s a little, triangular bone at the base of the spine, also known as the tailbone. This condition often results in discomfort and soreness in the tailbone region, making sitting or standing for an extended period uncomfortable. It can be driven by several different things, such as trauma, injury, or occasionally it develops without a known reason (idiopathic). The degree of coccydynia can vary, and it is normally treated conservatively. However, in some circumstances, more invasive methods may be required.
Anatomy of the coccyx
With three to five segments, the coccyx is a triangle bone. The largest and first segment connects with the sacrum, a bone supporting the pelvis. The final three segments of the tailbone typically join to create a single bone part and shrink in size.1
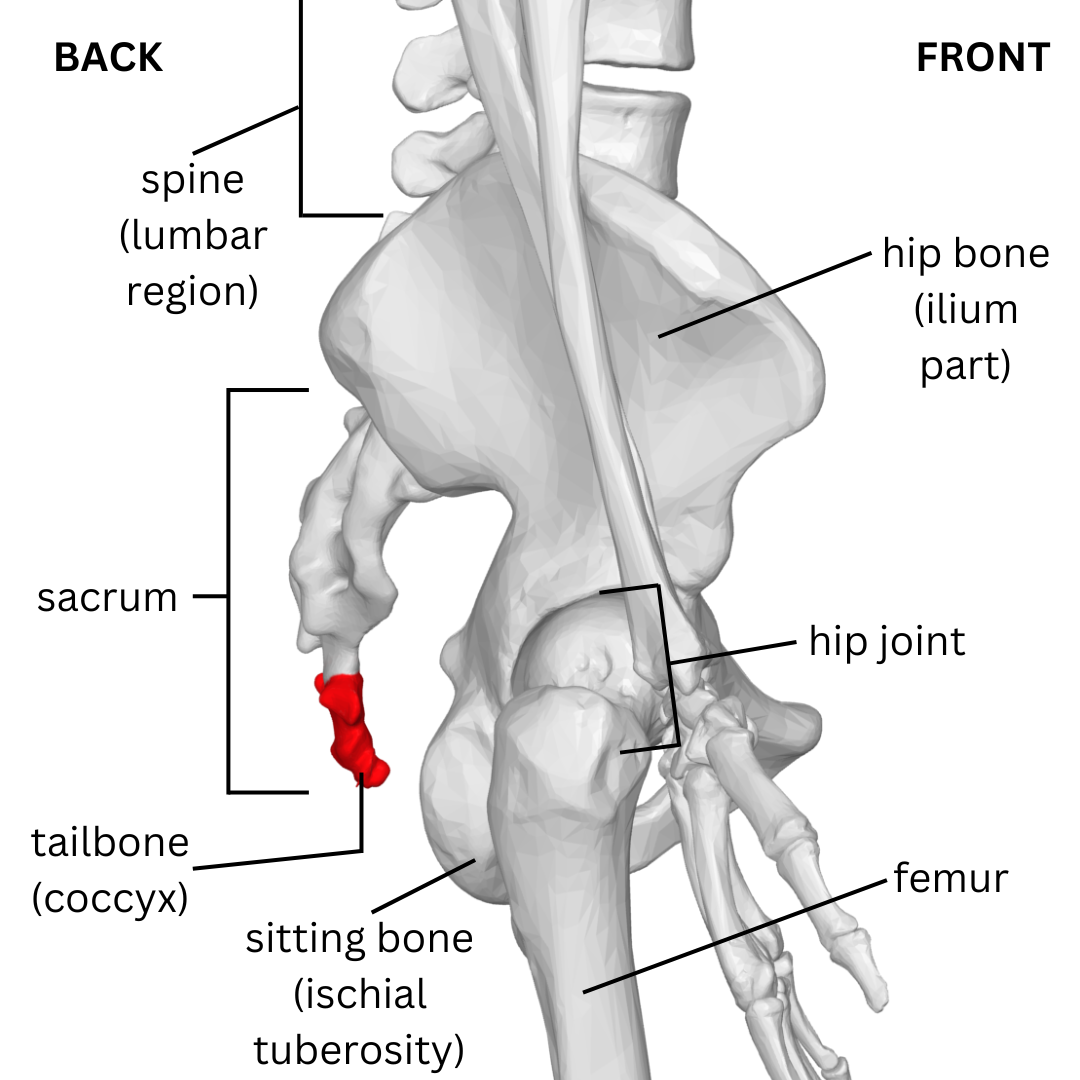
The side view of the pelvis and its bones, with the coccyx labelled in red. Created in Canva, adapted from Wikimedia Commons by Antonina Swierkowska.
The pelvic region is supported and stabilised by the coccyx, a significant but frequently disregarded component of the spine, which also serves as an attachment point for several muscles and ligaments. Lower back and buttock pain and discomfort may result from coccyx injuries or conditions, such as coccydynia.
Causes of coccydynia
The typical pain associated with coccydynia is caused by injury to the coccyx or coccygeal joints (joints of the tailbone). Other causes include:
- Inflammation of the surrounding tissue
- Contraction of the muscles connected to the coccyx2
- Dislocated or broken tailbone due to falls that land directly on the coccyx
- Accumulating strain to the tailbone, such as during long periods of sitting, especially on uncomfortable surfaces15
- Pregnancy and sitting incorrectly during the postpartum phase (after childbirth)3
- Tailbone morphology (shape)5
A body mass index (BMI) of greater than 27.4 for people assigned female at birth and 29.4 for people assigned male at birth was associated with a higher risk of developing posttraumatic (after injury) and idiopathic (of unknown cause) coccydynia. This is because the pelvis faces more backwards when obese patients try to sit down instead of being in a neutral position. This creates higher pressures in the pelvis, causing strain when sitting or after falling, which could lead to tailbone dislocation over time.4, 15
Another important cause of coccydynia is a retroverted coccyx, where the coccyx is partly pointing backwards instead of forwards and down, accompanied by a tiny pilonidal sinus pit and a palpable bony protuberance on the coccyx, called a spicule. Chronic accidental bursitis develops as a result of spicules irritating the coccygeal area when the patient is seated, especially if the coccyx is immobile.4
In a clinical study, 25% of the patients had coccygeal luxation predominantly in the sitting position, and 15 out of the 21 patients had positive results from provocative discography. This is a diagnostic procedure for spinal disc abnormalities, where a dye is injected into the intervertebral discs. The results suggested that coccygeal disc degeneration is most likely the source of the pain.6
Other rarer causes of coccydynia have been suggested by research. These include tuberculosis, deposits of calcium crystals in the joints of the coccyx, and tumours such as chordoma, trichoblastic carcinoma, and notochordal cell tumours. In addition, where the cause of pain could not be determined, it has been suggested that psychological origins should also be considered.7,8
Common symptoms
The primary complaints of patients with coccydynia include soreness and pain or an ache that is restricted to the lower sacrum, the coccyx, or the nearby soft tissues and muscles of the pelvis. The coccyx is typically indicated by the patient as the painful location. Several factors, including the amount of time spent sitting, affect how bad the pain is. People assigned female at birth report exponentially increased premenstrual pain during this time. Coccydynia has occasionally been linked to dyspareunia (painful sexual intercourse) and piriformis syndrome (a muscle pressing on the sciatic nerve). Additionally, patients who report pain during sexual activity or defecation seem to be more likely to experience levator muscle spasms, causing pain in the rectum and anus.9
Diagnosis
The majority of the evidence used to diagnose coccydynia comes from clinical examination using:
- Patient history to assess the levels of pain and its localisation, ruling out any differential diagnoses
- Physical examination, such as rectal examination to determine the range of motion of the coccyx15
- X-rays or CT scans to identify coccyx displacement or fractures.
- Routine blood tests could reveal the presence of a tumour or an infection.
Dynamic disorders like coccydynia are only fully understood by viewing dynamic films. Therefore, dynamic X-rays may be used to assess the movements of the coccyx, such as its increased (hypermobility) or decreased mobility (hypomobility).15
Evaluating the patient's coccygeal mobility is done by comparing static and dynamic radiographs, while the patient sat on a hard stool, causing increased pain, and with their hips flexed (with knees closer to the chest). To measure and compare the movement of the coccyx, the X-rays of a patient in both positions are put to overlap. Specialists make calculations for the angles, mobility and pelvic rotation (to the front and back) by measuring the difference between the coccyx tip on both films.6 The coccyx can be categorized as normal, subluxated (partially dislocated), immobile, or hypermobile based on its degree of mobility.6 Based on the description of the intercoccygeal angle (the angle of how curved the tailbone is to the front of the body) and the angle between the first and last segments of the coccyx, which was greater in patients with idiopathic coccydynia, it is possible to see the differences between traumatic and idiopathic (unknown) causes of coccydynia on a radiograph.10
Due to the dynamic nature of coccydynia, static MRI is unable to determine its cause.
Treatment options
A wide range of treatment approaches have been suggested to address coccydynia, such as:
- Hot baths
- Ring-shaped cushions, recommended when rectal pain is present, or C-shaped coccyx cushions to reduce pressure on the tailbone when sitting15
- Laxatives to relieve pain when passing stools
- Non-steroidal anti-inflammatory drugs (NSAIDs) for pain
- ergonomic modifications to physical therapy for the better sitting position
About 90% of patients respond well to conservative treatment.9, 11, 12 For example, the use of ergonomic adaptations such as cushions is widespread. The use of firm corsets or rubber rings, postural training, and buttock strapping are among the other conservative methods, but the evidence for their effectiveness is not very strong.
When the usual methods do not help with coccydynia, other types of treatments for the condition are available:
- Sacrococcygeal (in the area of the sacrum and coccyx) injections of steroids and local anaesthetics to reduce the pain
- Intrarectal massage and manipulation to try to improve coccyx alignment
- Psychotherapy to help with dealing with the condition
- Coccygeoplasty (treatment for broken tailbone)
- Radiofrequency ganglion blocks, in which a nerve is electrically stimulated to reduce sending pain signals to the brain, are used for cancer-related pain and severe cases of coccydynia for pain relief.
- Radiofrequency thermocoagulation, in which a nerve is damaged using heat, stops the information about the pain from being sent to the brain for long-lasting effects.
According to the nature of the underlying problem, pelvic floor muscle spasms are primarily responsible for pain, so manipulation therapy and massage can help with relaxing the muscles and reducing the pain. Steroid and local anaesthetic injections have grown in popularity as a form of treatment and as a way to identify patients who would benefit from coccygectomy.13
Moreover, instant pain relief was seen in a patient with a tailbone fracture after an injection of polymethylmethacrylate (PMMA) cement, also known as bone cement, usually used to stabilise the joints and bone fractures. 16 The process of bone cement injection is called coccygeoplasty. Another report revealed that a patient with coccydynia and dislocation of the coccyx could preserve its integrity by using Vicryl sutures (surgical, absorbable stitches) as a tension band.14
Patients who do not respond to conservative measures may undergo coccygectomy, which is the surgical removal of the coccyx, which is an ultimate option for very severe coccydynia.
Prognosis and recovery
It has been reported that patients who had coccygectomy (removal of the tailbone) for coccydynia had good to excellent outcomes. A good surgical outcome is more likely for coccydynia resulting from coccyx shape changes, the presence of the bursa, and a good response to injection.17
Coccydynia appears to be best managed with conservative measures like massage, injections, and ganglion impaction blocks. For patients with coccydynia, coccygectomy is an effective treatment option, particularly for those who meet certain criteria. Studies show that patients who have the right indications and undergo coccygectomy can have good or excellent outcomes, even though there seems to be a psychological component to the diagnosis.
Summary
The painful condition known as coccydynia is characterised by coccygeal pain, which is usually made worse by pressure. The perceived unpredictability of the pain's origin, certain psychological factors that may be connected to the condition, the availability of a variety of treatment options, and the inconsistent results all contribute to the uncertainty surrounding coccydynia.
If you suspect you have coccydynia or are experiencing coccyx pain, it's important to seek medical advice for a proper diagnosis and treatment plan tailored to your specific situation.
FAQs
How long does coccydynia last?
The duration of coccydynia varies from person to person. In many cases, it is a short-term condition that improves within a few weeks to a few months with conservative treatments. However, in some cases, it may become chronic and last for an extended period.
Can coccydynia be prevented?
While it may not always be preventable, there are steps individuals can take to reduce their risk of developing coccydynia, such as using proper ergonomics when sitting, avoiding prolonged sitting on hard surfaces, and taking breaks to stand and stretch during long periods of sitting.
Are there any complications associated with coccydynia?
In some cases, untreated or severe coccydynia can lead to chronic pain and may impact a person's quality of life. It can also affect posture and mobility.
Can coccydynia be related to other medical conditions?
Coccydynia can sometimes be associated with other conditions, such as pelvic floor dysfunction or conditions affecting the lower spine. It's essential to consult with a healthcare professional to rule out any underlying issues.
What exercises can help with coccydynia?
Physical therapy exercises can help strengthen or relax the pelvic floor and improve posture, which may alleviate coccydynia symptoms. These exercises should be prescribed and supervised by a healthcare professional.
References
- Pennekamp, Peter H., et al. “Coccygectomy for Coccygodynia: Does Pathogenesis Matter?:” The Journal of Trauma: Injury, Infection, and Critical Care, vol. 59, no. 6, Dec. 2005, pp. 1414–19. DOI.org (Crossref), https://doi.org/10.1097/01.ta.0000195878.50928.3c.
- Simpson, J. “INTRODUCTORY TO CLINICAL LECTURES ON THE DISEASES OF WOMEN.” The Lancet, vol. 115, no. 2944, Jan. 1880, pp. 155–57. DOI.org (Crossref), https://doi.org/10.1016/S0140-6736(02)31536-8.
- Schapiro, Saul. “Low Back and Rectal Pain from an Orthopedic and Proctologic Viewpoint with a Review of 180 Cases.” The American Journal of Surgery, vol. 79, no. 1, Jan. 1950, pp. 117–28. DOI.org (Crossref), https://doi.org/10.1016/0002-9610(50)90202-9.
- Maigne, Jean-Yves, et al. “Causes and Mechanisms of Common Coccydynia: Role of Body Mass Index and Coccygeal Trauma.” Spine, vol. 25, no. 23, Dec. 2000, pp. 3072–79. DOI.org (Crossref), https://doi.org/10.1097/00007632-200012010-00015.
- Postacchini, F., and M. Massobrio. “Idiopathic Coccygodynia. Analysis of Fifty-One Operative Cases and a Radiographic Study of the Normal Coccyx.:” The Journal of Bone & Joint Surgery, vol. 65, no. 8, Oct. 1983, pp. 1116–24. DOI.org (Crossref), https://doi.org/10.2106/00004623-198365080-00011.
- Maigne, Jean-Yves, et al. “Idiopathic Coccygodynia Lateral Roentgenograms in the Sitting Position and Coccygeal Discography:” Spine, vol. 19, no. 8, Apr. 1994, pp. 930–34. DOI.org (Crossref), https://doi.org/10.1097/00007632-199404150-00011.
- Powers, John A. “Coccygectomy:” Southern Medical Journal, vol. 50, no. 5, May 1957, pp. 675–78. DOI.org (Crossref), https://doi.org/10.1097/00007611-195705000-00024.
- Richette, Pascal, et al. “Coccydynia Related to Calcium Crystal Deposition:” Spine, vol. 33, no. 17, Aug. 2008, pp. E620–23. DOI.org (Crossref), https://doi.org/10.1097/BRS.0b013e31817c6cd2.
- Thiele, George H. “Coccygodynia: Cause and Treatment.” Diseases of the Colon & Rectum, vol. 6, no. 6, Nov. 1963, pp. 422–36. DOI.org (Crossref), https://doi.org/10.1007/BF02633479.
- Kim, Nam Hyun, and Kyung Soo Suk. “Clinical and Radiological Differences between Traumatic and Idiopathic Coccygodynia.” Yonsei Medical Journal, vol. 40, no. 3, 1999, p. 215. DOI.org (Crossref), https://doi.org/10.3349/ymj.1999.40.3.215.
- Sehirlioglu, Ali, et al. “Coccygectomy in the Surgical Treatment of Traumatic Coccygodynia.” Injury, vol. 38, no. 2, Feb. 2007, pp. 182–87. DOI.org (Crossref), https://doi.org/10.1016/j.injury.2006.09.013.
- Trollegaard, A. M., et al. “Coccygectomy: An Effective Treatment Option for Chronic Coccydynia: RETROSPECTIVE RESULTS IN 41 CONSECUTIVE PATIENTS.” The Journal of Bone and Joint Surgery. British Volume, vol. 92-B, no. 2, Feb. 2010, pp. 242–45. DOI.org (Crossref), https://doi.org/10.1302/0301-620X.92B2.23030.
- Plancarte, Drs. Ricardo, et al. “A751 PRESACRAL BLOCKADE OF THE GANGLION OF WALTHER (GANGLION IMPAR).” Anesthesiology, vol. 73, no. 3A, Sept. 1990, p. NA-NA. DOI.org (Crossref), https://doi.org/10.1097/00000542-199009001-00749.
- Bergkamp, Ab, and Ja Verhaar. “Dislocation of the Coccyx: A Case Report.” The Journal of Bone and Joint Surgery. British Volume, vol. 77-B, no. 5, Sept. 1995, pp. 831–32. DOI.org (Crossref), https://doi.org/10.1302/0301-620X.77B5.7559720.
- Buckland AJ, Burapachaisri A, Stekas N, Vasquez-Montes D, Protopsaltis T, Vigdorchik J. Obesity Alters Spinopelvic Alignment Changes From Standing to Relaxed Sitting: the Influence of the Soft-tissue Envelope. Arthroplasty Today [Internet]. 2020 [cited 2024 Mar 11]; 6(3):590-595.e1. Available from: https://www.sciencedirect.com/science/article/pii/S2352344120300248
- Dean LM, Syed MI, Jan SA, Patel NA, Shaikh A, Morar K, et al. Coccygeoplasty: Treatment for Fractures of the Coccyx. Journal of Vascular and Interventional Radiology [Internet]. 2006 [cited 2024 Mar 11]; 17(5):909–12. Available from: https://www.sciencedirect.com/science/article/pii/S105104430760832X.
- Kwon HD, Schrot RJ, Kerr EE, Kim KD. Coccygodynia and Coccygectomy. Korean J Spine [Internet]. 2012 [cited 2024 Mar 11]; 9(4):326–33. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4430558/.




