

Overview
Cancer can appear in one or both of the tubes that connect the ovaries and the uterus. These tubes are known as the fallopian tubes (or uterine tubes or oviducts). The cells lining the fallopian tubes are the site of over 95% of cancers. These oviducts are a pair of long, thin, hollow tubes on either side of the uterus. They are 11 to 12 cm long, with the central opening measuring less than 1 mm. These tubes are seromuscular organs that originate from the uterine “side” horns at the top of the uterus and extend laterally, i.e. towards the outer left and right sides of the body. The tubes end close to the ovary, situated on the same side. The fallopian tube comprises four anatomical areas located increasingly further away from the main uterus structure: uterine, isthmus, ampulla, and infundibulum. The uterine part of the fallopian tube is located nearest to the uterus. The ampulla, a common site for fertilisation, is located beside the isthmus and is a little farther away from the uterus. The infundibulum lies the furthest away from the uterus and finishes at an abdominal ostium that opens into the peritoneal cavity and fimbriae, which collect the released immature egg or germ cell (also known as an oocyte) during each menstrual cycle. The interior of the infundibulum is connected to the adjacent ovary by one fimbria, known as the fimbria ovarica. The fallopian tubes serve as
both a place for fertilisation and a pathway for the fertilised egg (known as an ovum or gamete) to travel from the ovary to the uterus.1,2
In those assigned female at birth (AFAB), ovarian, fallopian tube, and primary peritoneal carcinomas collectively account for 2.5% of all new instances of cancer in the United States (11.6 new cases per 100,000 AFAB annually, or more than 22,000 diagnoses). Despite being relatively uncommon, epithelial ovarian cancer is the fifth-leading cause of cancer-related mortality, accounting for more than 14,000 deaths yearly (7.2 deaths per 100,000). A total of 4,500 cases of epithelial ovarian cancer (EOC) and 40 cases of primary fallopian tube carcinoma (PFTC) are documented annually in England and Wales. Unfortunately, because there are not many effective screening methods, most diagnoses occur in the advanced stages of the disease, where the 5-year survival rate is less than 30%. Fallopian tube cancer typically occurs in women between 40–60 years of age, though some cases have been reported at an earlier age.3,4
Credits: https://www.histology.leeds.ac.uk/female/oviduct.php
Causes and types of fallopian tube cancer
The possible causes of fallopian tube cancer are, so far, unidentified. Hormonal, reproductive, and even genetic variables are known to raise the risk of EOC and PFTC.
High parity proved protective, and the use of oral contraceptives and a history of pregnancies also reduced the incidence of PFTC. Infertility, pelvic inflammatory disease (PID), prior hysterectomy, endometriosis, lactose intolerance, age, race, weight, and smoking had no significant association with PFTC. In fact, the development of cancer in both fallopian tubes was five times more in infertile compared to fertile patients. Women who had never had children (nulliparous) had a better prognosis than those who had children. There may even be molecular similarities between breast, serous ovarian, uterine carcinomas, and PFTC due to the frequency and structure of the chromosomal abnormalities (BRCA-1 or BRCA-2 mutations) seen in PFTC.4 Looking at fallopian cancer itself, there are different types of fallopian tube cancer, and the image below highlights these differences: The image below shows different types
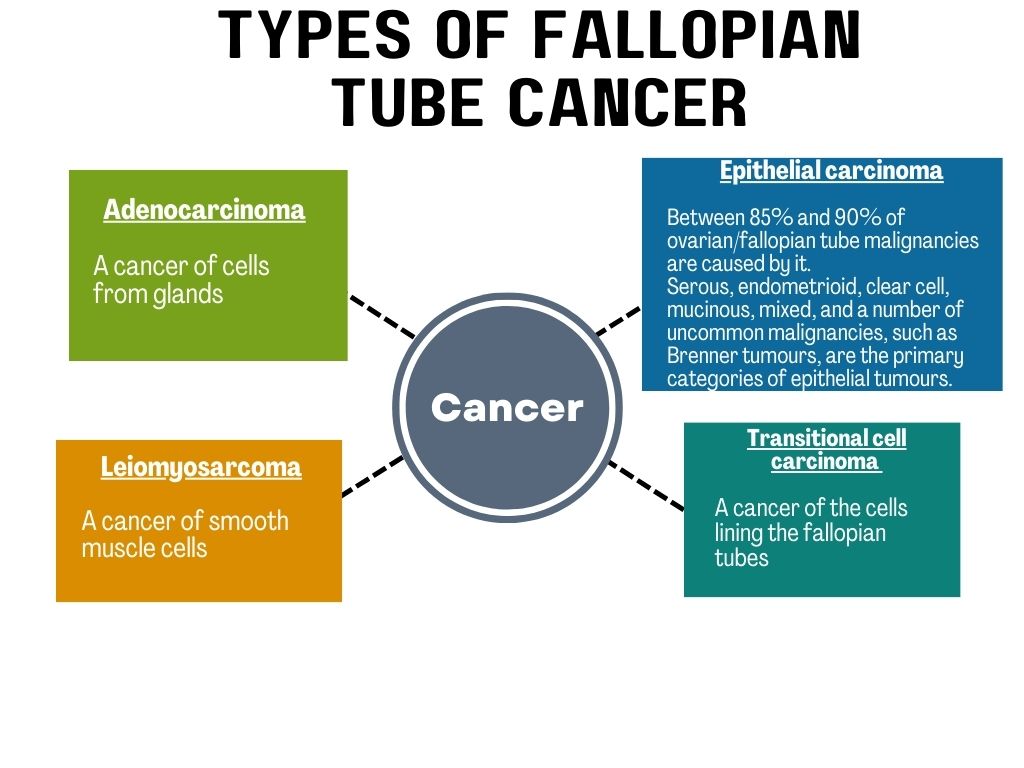
Adenocarcinoma, Brenner tumours, Leiomyosarcoma, Transitional cell carcinoma
Signs and symptoms
Often, there are no early warning signs or symptoms for ovarian, fallopian tube, or peritoneal cancer. When signs or symptoms do
appear, the cancer is frequently at an advanced stage. The following are possible signs and symptoms:-
- Bleeding or spotting from the vagina
- Pain in the abdomen, whether colicky or dull
- Pelvic or abdominal mass
- Ascites
- Uncommon manifestations (acute abdomen, a palpable nodule in the groin area (inguinal node), umbilical-bone cerebral metastases, and cerebellar degeneration)
- Postmenopausal bleeding or spotting with a negative PAP smear
- 15% of instances documented have what is known as the “Latzko's triad of symptoms”, which include irregular, profuse serosanguinous vaginal discharge, colicky pain relieved by discharge, and abdominal or pelvic mass.4,7
Diagnosis
The combination of the following diagnostic techniques detects the possibility of fallopian tube cancer:
- Medical history and physical examinations
A complete medical history is required to identify any potential risk factors with any history of cancer. The next step is to conduct a blood test and thorough physical examinations of the breast, pelvic (including a pap test), and rectal areas.
- Imaging tests
Computed tomography (CT scan) of the abdomen and pelvis identifies the degree of intra-abdominal disease. Transvaginal ultrasound produces pictures of the pelvis using sound waves. Magnetic resonance imaging (MRI) yields more precise imaging of the reproductive organs.
- Biopsy
Suspected lesions, lumps, or adhesions are examined with a biopsy or surgical excision. Peritoneal biopsies from random surfaces of the peritoneum, including those from the right side of the underside of the hemidiaphragm, the bladder reflection, the cul-de-sac, the right and left paracolic recesses, and pelvic sidewalls.
This step helps to determine the extent and spread of the disease. Patients with early-stage or advanced-stage disease experience symptoms that are frequently very subtle and have similar symptom durations.
- Tumour markers
Your physician will consider tumour markers such as CA125 and carcinoembryonic antigen (CEA). Epithelial ovarian, fallopian tube or peritoneal cancers will be the most typical diagnoses if there is a high CA125 level.
- Genetic testing
Inherited gene mutations feature in approximately 20% of ovarian, fallopian tube, and peritoneal cancers. Genetic testing can identify genetic mutations like BRCA1 or BRCA2 that can affect treatment options.8
Management and treatment
The management and treatment of fallopian tube cancer depends on many factors, such as the stage of the disease, type, the patient's general health, and personal preferences. A brief description of fallopian tube cancer management and treatment options follows :
Surgery
The type of surgery is based on the cancer's stage, determined by imaging studies. Treatment for early-stage fallopian tube cancer involves a salpingo-oophorectomy. It entails removing one or both ovaries with one or both fallopian tubes. In more advanced cancer stages, you might also require a total abdominal hysterectomy (removal of the uterus), bilateral salpingo-oophorectomy, infrasonic omentectomy (removal of the abdominal lining), appendectomy (removal of the appendix), peritoneal washings, and peritoneal biopsies. The objective is to eradicate all possible cancer from patients with advanced disease. Surgery will involve either radiation therapy or chemotherapy afterward. This is also known as adjuvant therapy. Staging and tumour debulking are two objectives of surgical intervention.
Radiation therapy
High-energy X-rays serve to kill cancer cells in this procedure. For fallopian tube cancer, radiation is not the main course of treatment. The adverse effects are frequent, and it could be more effective. It also helps the tumour shrink before surgery.
Chemotherapy and targeted therapies
Chemotherapy can be used following surgery to eradicate cancer cells that may remain. Recurrent or advanced fallopian tube cancer is treated with targeted therapies. The following table shows suggested interventions for various phases.
| Stages of fallopian tube cancer | Suggested treatment |
| Stage I | Carboplatin AUC (area under the curve) 5-7.5 IV injected over 30-60 min every 21 days for three to six cycles with paclitaxel 135-175 mg/m2 IV infused over 3 hours or Docetaxel 60–75 mg/m2 IV, administered over 1 hour in addition to carboplatin AUC 5–6 IV injected over 1 hour every 21 days for three–six cycles. |
| Stage II-III | Paclitaxel 60 mg/m2 IP (intraperitoneal) on the 8th day every 21 days for six cycles, followed by cisplatin 100 mg/m2 IP on day 2 (which is lowered to 75 mg/m2 and administered on day 1 or 2 to allow an outpatient regimen). Paclitaxel 135 mg/m2 IV (intravenous) infused over 24 hours on day 1 (maybe given over 3 hours if tolerated). |
| Stage II-IV | Paclitaxel 135-175 mg/m2 IV given over 3 hours with carboplatin AUC 5-7.5 IV infused over 30-60 min every 21 days for six cycles or every 21 days for six cycles, administer dose-dense paclitaxel 80 mg/m2 IV days 1,8, and 15 with the administration of carboplatin AUC 5–6 IV Day 1 or Docetaxel 60-75 mg/m2 infused over 1 hour plus carboplatin AUC 5-6 IV infused over 1 hour every 21 days for three to six cycles. |
| Recurrent (platinum-sensitive) disease | Doxorubicin 30 mg/m2 IV given over 30 min in addition to carboplatin AUC 5 IV every 21 days for six cycles or Gemcitabine 1000 mg/m2 IV on days 1 and 8 with carboplatin AUC 4 on 1st day every 21 days for six cycles or every three weeks, paclitaxel 80 mg/m2 IV is administered over three hours, along with a push of carboplatin AUC 6 IV or Bevacizumab (15 mg/kg IV on day 1) plus carboplatin IV (AUC 5 on day 1) plus paclitaxel (175 mg/m2 IV on day 1) and gemcitabine (1000 mg/m2 IV on days 1 and 8) every 21 days for six to eight cycles, followed by continued use of Bevacizumab 15 mg/kg every 21 days as a single agent. |
| Recurrent (platinum-resistant) disease | Topotecan 1.25 mg/m2 IV infused over 30 minutes on days 1–5 every 21 days or Pegylated Liposomal Doxorubicin 50 mg/m2 IV infused over 30 minutes every 21 days or Gemcitabine 1000 mg/m2 IV infusions lasting 30 minutes every 21 days on days 1 and 8.10,11 |
Talk with your healthcare provider about your treatment options, including any potentially positive and negative aspects. Personalised treatment plans are created according to each patient's unique diagnosis and situation.
Prevention
Since the specific causes are not entirely understood and some risk factors, such as genetic abnormalities, are uncontrollable, preventing fallopian tube cancer might be difficult. The American Cancer Society recommends genetic testing for women who have a known family history of the BRCA mutation, women who have been diagnosed with ovarian cancer, pancreatic cancer, breast cancer at a younger age, more than one family member with breast cancer, and breast cancer in a male family member. It is also possible to do genetic testing to detect sporadic mutations or any familial genetic mutations. The ovarian, fallopian tube and peritoneal malignancies have no known screening techniques that lower mortality rates. It is more probable to have false-positive results leading to unnecessary interventions because disease frequency is low and there aren't many high-quality screening tools available. Early detection by routine check-ups and heightened symptom awareness are crucial in controlling the disease.8,12
FAQs
Is fallopian tube cancer aggressive?
A relatively aggressive gynaecological cancer is PFTC. One per cent of all female genital malignancies arise from it.9
How long does a person with fallopian tube cancer survive?
Patients with PFTC have a 22–57% 5-year overall survival rate. To predict patient outcomes more accurately, some prognostic indicators are studied. Stage, patient age, and the presence of a residual tumour following the initial operation are all consistently significant prognostic markers.13
Does removing fallopian tubes reduce cancer risk?
The likelihood of ovarian cancer is reduced by performing salpingectomy when individuals undergo surgery e.g. hysterectomy. Opportunistic salpingectomy has the potential to dramatically lower the risk of ovarian cancer, although it doesn't eliminate it.14
Summary
Effective management of fallopian tube cancer depends on early identification and immediate medical care. Consulting a healthcare expert is crucial if you have symptoms or risk factors. People diagnosed with fallopian tube cancer early, before the disease extends outside the pelvic area, have a good prognosis.
References
- Jean Hailes for Women’s Health. Fallopian tube cancer. [Internet]. Australia Jean Hailes Foundation [updated: 2023 Apr 14; cited 2023 Sep 4]. Available from: https://www.jeanhailes.org.au/health-a-z/ovaries-uterus/gynaecological-cancers-ovaries-and-uterus/fallopian-tube-cancer
- Han J, Sadiq NM. Anatomy, abdomen and pelvis: fallopian tube. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [update: 2023 Jul 24; cited 2023 Sep 4]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK547660/
- Stasenko M, Fillipova O, Tew WP. Fallopian tube carcinoma. JOP [Internet]. 2019 Jul [cited 2023 Sep 4];15(7):375–82. Available from: https://ascopubs.org/doi/10.1200/JOP.18.00662
- Pectasides D, Pectasides E, Economopoulos T. Fallopian Tube Carcinoma: A Review | The Oncologist | Oxford Academic [Internet]. OUP Academic. Oxford University Press; 2006 [cited 2023 Sep 5]. Available from: https://academic.oup.com/oncolo/article/11/8/902/6397105
- Cancer.Net [Internet]. 2012 [cited 2023 Sep 5]. Ovarian, fallopian tube, and peritoneal cancer - introduction. Available from: https://www.cancer.net/cancer-types/ovarian-fallopian-tube-and-peritoneal-cancer/introduction
- GARD Rare disease information - fallopian tube cancer - national organisation for rare disorders [Internet]. 2022 [cited 2023 Sep 5]. Available from: https://rarediseases.org/gard-rare-disease/fallopian-tube-cancer/
- PDQ Adult Treatment Editorial Board. Ovarian epithelial, fallopian tube, and primary peritoneal cancer treatment (Pdq®): patient version. In: PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute (US); 2002 [cited 2023 Sep 5]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK65718/
- Berek JS, Renz M, Kehoe S, Kumar L, Friedlander M. Cancer of the ovary, fallopian tube, and peritoneum: 2021 update. Intl J Gynecology & Obste [Internet]. 2021 Oct [cited 2023 Sep 6];155(S1):61–85. Available from: https://obgyn.onlinelibrary.wiley.com/doi/10.1002/ijgo.13878
- Zardawi IM. Primary fallopian tube carcinoma arising in the setting of chronic pelvic inflammatory disease. Case Rep Med [Internet]. 2014 [cited 2023 Sep 6];2014:645045. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3913490/
- Fallopian tube cancer treatment protocols: treatment protocols. 2022 Apr 8 [cited 2023 Sep 7]; Available from: https://emedicine.medscape.com/article/2056981-overview
- Fallopian tube cancer: staging and treatment | oncolink [Internet]. [cited 2023 Sep 7]. Available from: https://www.oncolink.org/cancers/gynecologic/fallopian-tube-cancer/fallopian-tube-cancer-staging-and-treatment
- Hundal J, Lopetegui-Lia N, Rabitaille W. Fallopian tube cancer– challenging to diagnose but not as infrequent as originally thought. Journal of Community Hospital Internal Medicine Perspectives [Internet]. 2021 May 4 [cited 2023 Sep 7];11(3):393–6. Available from: https://www.tandfonline.com/doi/full/10.1080/20009666.2021.1893889
- Akkaya E, Sanci M, Kulhan NG, Kulhan M, Nayki U, Nayki C, et al. Prognostic factors of primary fallopian tube carcinoma. Contemp Oncol (Pozn) [Internet]. 2018 [cited 2023 Sep 7];22(2):99–104. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6103229/
- American College of Obstetricians and Gynecologists. Opportunistic salpingectomy as a strategy for epithelial ovarian cancer prevention [Internet]. [cited 2023 Sep 7]. Available from: https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2019/04/opportunistic-salpingectomy-as-a-strategy-for-epithelial-ovarian-cancer-prevention




