

Overview
Cancer, a life-changing condition, presents in many forms, sometimes with bumps or lumps on the body, sometimes as fatigue and fever or sometimes as night sweats and weight loss. What it generally means is that when the DNA of a single cell changes (mutates), that cell can’t develop and function normally. Cancer has many different types and can affect different tissues; in this post, we will be talking about cancer that affects the blood, called ‘’leukaemia’’.
Leukaemia is a disease of the blood, derived from the Greek words ‘’Leukos,’’ meaning white and ‘’Haima’’ meaning blood. It is a type of cancer that affects your blood. It usually begins in the bone marrow, where most of the blood components are made, thus resulting in a high number of abnormal blood cells. Leukaemia also has different types; some affect children more, others occur mostly in adults. In leukaemia, the white blood cells, which are infection fighters, are not working properly and are being excessively produced.1
Leukaemia is classified based on onset and cell type as follows:1
- Acute lymphocytic leukaemia (lymphatic) - (ALL)
- Acute myelocytic leukaemia (Bone marrow) - (AML)
- Chronic lymphocytic leukaemia (lymphatic) - (CLL)
- Chronic myelocytic leukaemia (Bone marrow) - (CML)
Here, we discuss Large Granular Lymphocytic Leukaemia (LGL) which is a subtype of Chronic Lymphocytic Leukaemia (CLL). LGL is a rare type of chronic leukaemia and grows slowly. It typically affects people aged 60 and older. Treatment for LGL is available but as of currently, there is no cure.2
Understanding Leukaemia and LGL is important for many reasons, and in this article, we touch on those topics so that you can get all the information you require to make informed decisions. A new diagnosis comes with lots of uncertainty, and this can be due to emotional stress, treatment decision-making, physical and symptom management, lifestyle adjustments, and support networks. All these require understanding and a certain amount of foresight.
Causes of large granular lymphocytic leukemia
When speaking of leukaemia, many genetic and environmental risk factors are identified in the development of leukaemia, which are as follows:1
- Radiation exposure - people who have had certain types of chemotherapy and radiation therapy for other cancers have an increased risk of developing certain types of leukaemia.
- Alkylating agent exposure - exposure to certain chemicals like benzene and formaldehyde found in building materials and household chemicals.
- Family history - research suggests that some types of leukaemia may run in families. In most cases, however, having a genetic history doesn’t necessitate that other family members will also develop leukaemia.
- Viral infections - research has associated LGL with the Human T-Lymphotropic Virus (HTLV1) infections, leading to malignant mutations the most. Other viral relationships have also been established namely with Hepatitis C Virus, Epstein Barr Virus, and Cytomegalovirus.
- Smoking - If you have a history of smoking or exposure to second-hand smoke, then you're at risk of AML.
- Genetic syndromes (like Downs syndrome, Fanconi anaemia, and Li-Fraumeni syndrome) may increase your risk.
Generally speaking, the exact cause of LGL leukaemia is not known and is usually traced down to a mutation in the genetic material leading to the malignant transformation of hematopoietic (blood-forming) stem cells. Researchers believe that a viable link is present between this leukaemia and immune response, autoimmune diseases and other cancers. In leukaemias, these malignant cells are generally immature, poorly differentiated, abnormal white cells, also called blasts (i.e. are still young in their maturation process) that can either be lymphoblasts or myeloblasts.
Large Granular Lymphocytic leukaemia is rare and is caused by dysregulation in pathways that cause cellular death when a mutation is detected. There are multiple pathways that regulate this cellular death, like the JAK-STAT3 pathway or the JAK-STAT5B pathway.2
Signs and symptoms of large granular lymphocytic leukemia
Some people with this illness may never exhibit any symptoms. According to one study, around one-third of LGL patients had no symptoms at the time of their diagnosis. Instead, blood testing revealed they had abnormally low quantities of red blood cells or neutrophils (a type of granular white cell), which is how they discovered they had LGL. When someone is receiving treatment for a blood condition and exhibits symptoms that doctors believe are consistent with large granular lymphocytic leukaemia, they may be diagnosed with LGL. Those who do experience symptoms frequently exhibit the following:
- Frequent fevers and recurrent illness
- Fatigue
- Enlarged spleen
LGL is commonly seen in people in their 70s. As part of the disease manifestation, people usually are not symptomatic (as mentioned above). One-third of those that are usually only present with fatigue. People present with fatigue due to decreased red blood cells, whereas fever and recurrent illness are due to decreased white blood cells known as neutrophils. The enlarged spleen is due to an increase in the number of immature white cells that are filtered by the spleen.
Apart from the above signs and symptoms, studies have found that LGL leukaemia is frequently associated with autoimmune disorders, with Rheumatoid arthritis being the most common association. Other associations are ulcerative colitis, Sjogren syndrome, and Systemic Lupus Erythematosus. These can present with bowel movement problems, skin manifestations, dry eyes, skin & mouth, muscle & joint pain etc.2
Diagnosis
Clinical suspicion and reasoning are very important in diagnosing especially, in cases of unexplained neutropenia, recurrent infections, anaemia, lymphocytosis or autoimmune conditions.
Blood testing and genetic analysis are frequently used by medical professionals to diagnose this illness. Typical testing includes:
- Complete blood count (CBC) with differential: The number of each type of white blood cell is counted as part of a CBC with differential.
- Peripheral blood smear: Medical professionals can count the quantity of LGLs in your blood by closely examining blood cells under a microscope.
- Flow cytometry: This laboratory procedure examines cell properties. This test is frequently used by doctors to identify and categorise different kinds of leukaemia.
- Immunophenotyping: Medical professionals look for markers on cell surfaces in blood or tissue samples. Markers identify particular varieties of certain conditions.
- Analysis of T-cell receptor (TCR) gene rearrangements: These blood or bone marrow tests are used by medical professionals to check for issues with the genes that govern how your T-cells function.
- Gene testing: Look for STAT3 or STAT5 gene mutations, which can lead to leukaemias.
In order to rule out illnesses, including immunodeficiency, rheumatoid arthritis, myelodysplasia, and myeloid mutations, they may perform additional testing, such as bone marrow analyses. They might also examine the amounts of monoclonal proteins and immunoglobulins, which are products produced by the white blood cells to help detect and fight foreign/abnormal presence in the body.2
Management and treatment for LGL
When dealing with cancer, management usually involves a team of specialists. This is what is referred to as a multidisciplinary team (MDT) in the medical field. There are many issues that the team helps you deal with; these include emotions, support, lifestyle adjustment, survivorship and advanced cancer.
Dealing with these is just as important as it is to deal with cancer using pharmacotherapy and adjunct therapies. During treatment, you’ll be seen by the doctor and nurse regularly; how often depends on the stage of your cancer and how you are feeling before receiving each cycle.
The different types of approaches that are used include; watchful waiting, targeted therapy, chemotherapy, radiation therapy, immunotherapy and chemotherapy with bone marrow or peripheral blood stem cell transplant.
We will first discuss medical treatment in LGL. These cases, even though asymptomatic, eventually will need treatment as they become symptomatic over time. The indication for starting treatment is usually based on blood counts of white blood cells called neutrophils; severe neutropenia (<500 cells/uL), along with infection, is what is required for initiation.2
The medications used are as follows;
- Steroids: Although steroids can improve neutropenia and alleviate certain symptoms, remissions are typically short-lived, and patients eventually experience the negative effects of steroid medication.
- Oral Methotrexate: When administered at a level of 10 mg/m2 orally once a week, it is one of the best treatments for neutropenia. The average length of therapy is 1 to 9 years. Regular hepatic and renal check-ups are necessary because it interfere with liver and renal function as a side effect.
- Cyclosporin: Can be used alone or in combination with steroid or methotrexate as a first-line or second-line medication. It is taken orally twice a day at a dose of 1-1.5 mg/kg. Since the response is not long-lasting and relapses can happen after stopping, ongoing administration is necessary.
- Cyclophosphamide: An oral dose of 50–100 mg/day of the alkylating drug cyclophosphamide can be used effectively in circumstances where other treatments have failed. Compared to methotrexate, it has a better impact on neutropenia, albeit the response is not long-lasting, and the illness could return if treatment is discontinued. It has adverse consequences, such as myelosuppression, which needs growth factor supplementation. For non-responders, it should be used for no more than 4 months, and for respondents, it should be used for between 6 and 12 months. Regular monitoring of renal function is necessary.
Previously, LGL was treated with polychemotherapy like CHOP (cyclophosphamide, doxorubicin, vincristine and prednisone) or CVP (cyclophosphamide, vincristine and prednisone) based therapies which were associated with poor prognosis. Apart from chemotherapy, other treatments like radiotherapy and surgery are rarely implemented in chronic leukaemias.2
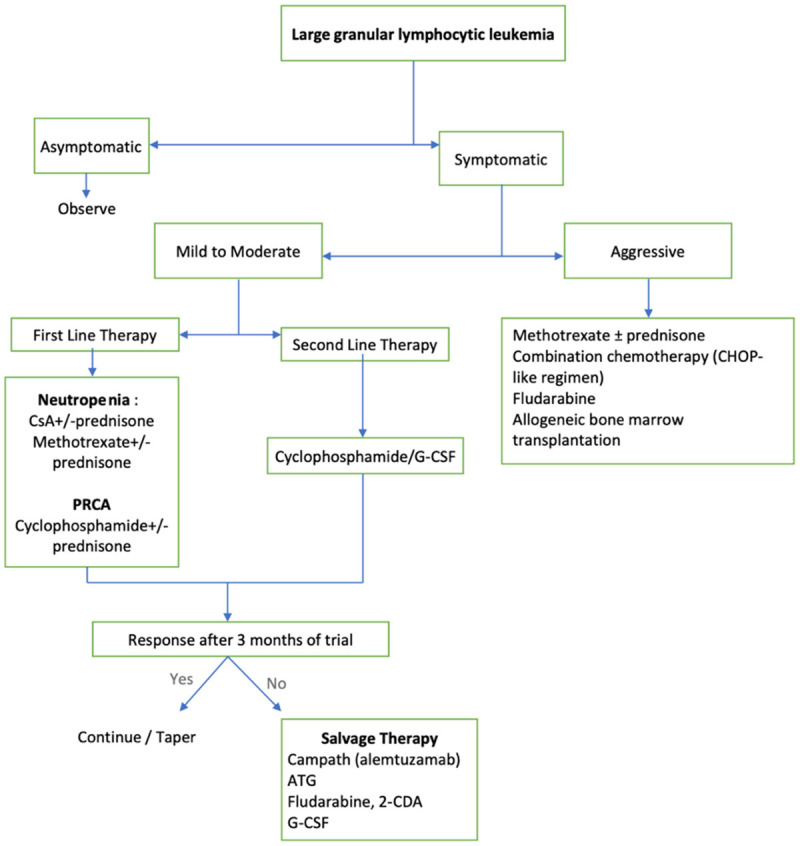
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8918699/bin/ajbr0012-0017-f4.jpg
Other aspects of the treatment include:
- Supportive treatments - medicines to prevent infections, blood or platelet transfusions, and vaccines. Improving quality of life is a vital principle that is focused on here.
- Side Effects treatment - medication for side effects of chemotherapy. Please speak to your doctor about side effects, at any time during your treatment.
- Emotional & Mental Support - for this your specialist could refer you or have a psychiatrist and psychologist incorporated as part of the team so that you can know what to expect and how to deal with the stressful situations you might find yourself in. Another aspect of this is going to local support groups and meeting people with similar experiences. Your nurse specialist can give you more information on different support groups.
- Community support - occupational therapy and physiotherapy are important aspects of this form of therapy. Therapists come to your home and make adjustments, whereas physiotherapists help with coping with side effects physically. Apart from this, it also involves building connections with family and other patients.
FAQs
How can I prevent large granular lymphocytic leukaemia?
You cannot prevent developing large granular lymphocytic leukaemia since healthcare workers don't know what exactly causes it. However, people with autoimmune disease have an increased risk of developing LGL; ask your doctor whether you should be concerned.
How common is large granular lymphocytic leukaemia?
LGL is a rare disorder, constituting 2-5% of all chronic lymphoproliferative diseases in the US and Europe and 5-6% of all cases in the Asian population. Recent demographic studies of European and North American cohorts place the average incidence of LGL leukaemia at 0.2-0.72 per million per year.2
Who is at risk of large granular lymphocytic leukaemia?
The exact cause has not been established, but certain risks have been shown to be associated. People with autoimmune disorders have been seen to be at higher risk, along with exposure to carcinogenic agents like ones present in smoke and alkylating agents in building and household chemicals.
What can I expect if I have LGL?
People with LGL can typically live the same lifespan as people who don’t have the condition. But, what really gets affected is the quality of life.
When should I see a doctor?
You should see your doctor if you develop symptoms. If you have symptoms and are receiving treatment, and you notice changes in your body that make you feel worse, then please go and see your doctor.
Summary
White blood cells are impacted by the rare blood malignancy known as large granular lymphocytic leukaemia (LGL). Even if you have this ailment, you might not notice any physical changes that could represent LGL symptoms. Sometimes, people may go years without experiencing symptoms. Although the illness cannot be cured, healthcare professionals have methods to control its symptoms. Hearing that you have an incurable illness could be frightening. Your medical professionals will comprehend why you might be concerned about what comes next. They'll be happy to go over what you can do right away to support your health as well as what to anticipate if you do start to experience symptoms. It could make you feel more at ease about residing with LGL if you know what to anticipate.
References
- Chennamadhavuni A, Lyengar V, Mukkamalla SKR, Shimanovsky A. Leukemia. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Jul 17]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK560490/
- Rahul E, Ningombam A, Acharya S, Tanwar P, Ranjan A, Chopra A. Large granular lymphocytic leukemia: a brief review. Am J Blood Res [Internet]. 2022 Feb 15 [cited 2023 Jul 17];12(1):17–32. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8918699/




