 Medical contributor:
Medical contributor: First revision:
First revision: Mirizzi syndrome: What is it? You may be wondering what this condition is about. Let's evaluate it beginning with the following mnemonic that can describe the syndrome:
- M - Mucus-filled bile ducts
- I - Impacted Gallstone
- R - Right upper quadrant pain
- I - Icterus (jaundice)
- Z - Zipper-like appearance on imaging
- Z - Z-compression of the bile duct
- I - Infection
Mirizzi syndrome is an unusual consequence of persistent gallstone disease, caused by obstruction when a big gallstone or cluster of stones becomes lodged in the gallbladder or cystic duct and grows enough to compress another duct from the outside. This then blocks the flow of bile, which is crucial for emulsifying fats.
It can be difficult to perform surgery for Mirizzi syndrome as the anatomy involved can be difficult to see in advance. This article will provide you with a better understanding of the disease so you can seek medical attention quickly if appropriate.
Overview
Mirizzi syndrome is a rare form of obstructive jaundice (yellowing of the skin) caused by the extrinsic constriction of an extrahepatic biliary channel in the cystic duct or gallbladder. Although it is a functional hepatic condition, it is often associated with biliary channel dilatation and can mimic other hepatobiliary diseases, such as cholangiocarcinoma. For example, Jaundice can cause similar symptoms of other conditions, such as ascending cholangitis (infection of the biliary tree) and common bile duct stones to be confused with cholecystitis (inflammation of the gallbladder). The majority of gallstones have no symptoms. Gallstones affect roughly 14 million people assigned males at birth (AMAB) and 6 million people assigned females at birth (AFAB) in the US, ranging in age from 20 to 74. As a person ages, the prevalence rises. Three of the usually frequent complications of chronic gallstone diseases are acute pancreatitis, cholangitis, and cholecystitis. Other benign problems like Mirizzi syndrome and gallstone ileus are usually uncommon. Obesity, as well as those who are underweight, runs a higher risk of acquiring gallstones. In addition, hormones also affect gallstones and Mirizzi Syndrome. Oestrogen is shown to increase bile cholesterol and decrease gallbladder contractility. In contrast to those AMAB men, the production of gallstones is two times more likely in AFAB women of reproductive age or those taking oestrogen-containing birth control. Due to neuropathy (damaged nerves) in chronic conditions such as diabetes, more gallstones can develop and there can be less contraction in their gallbladder walls.1,2
Causes of Mirizzi syndrome
As mentioned, Mirizzi syndrome is caused by the extrinsic constriction of an extrahepatic biliary channel by one or more gallstones in Hartmann's pouch, the gallbladder infundibulum, or the cystic duct.
The external compression of the bile duct and the later development of cholecystobiliary (an impacted stone that has damaged the cystic duct (CD) and is eroding into the common hepatic duct (CHD)) and cholecystoenteric fistulas (between an inflamed gallbladder and one or more regions of the gastrointestinal system around it) appear to be distinct stages of the same disease process in the current understanding of Mirizzi syndrome.
Long cystic ducts that parallel the bile duct and a low insertion of the cystic duct into the bile duct are also associated with the development of Mirizzi syndrome. Gallstone impaction that occurs frequently will result in recurrent attacks of acute cholecystitis and cause the gallbladder to become first enlarged with thick inflammatory walls. The gallbladder will eventually atrophy and contract, developing thicker fibrotic walls when it stays contracted. The bile duct and the gallbladder's proximity may cause oedematous inflammatory tissue to fuse with the gallbladder's walls and eventually become fibrotic, compressing the bile duct externally. Specifics of the Mirizzi syndrome's "anatomy" are shown in the picture below:
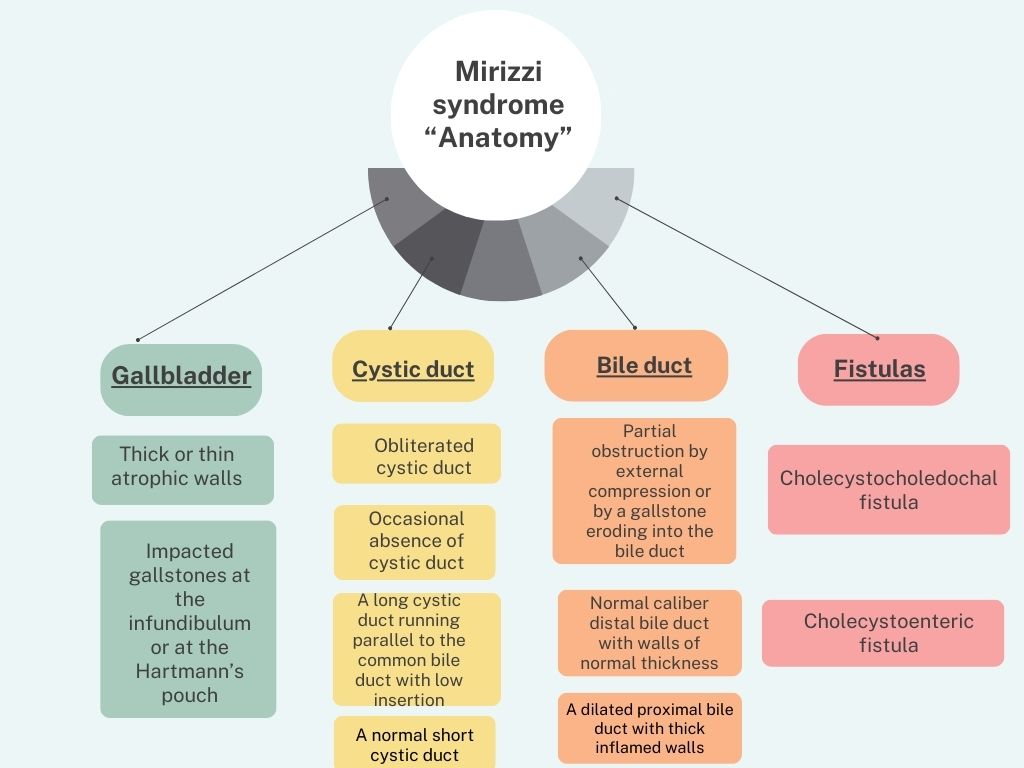
Created by: Deepika Rana
The Csendes classification system for Mirizzi Syndrome is the most well-known stratification system, although other categorisation schemes have been proposed. The Csendes system distinguishes five main kinds of Mirizzi syndrome.
| TYPE | DESCRIPTION |
| Type I | External compression on the common biliary duct (CBD) |
| Type II | Less than one-third of the CBD is affected by cholecystocholedochal fistula (gallstone erodes into bile duct) |
| Type III | Up to two-thirds of the CBD may be affected by a cholecystocholedochal fistula. |
| Type IV | Cholecystocholedochal fistula with total CBD wall deterioration |
| Type V | Cholecystoenteric fistula in types I–IV |
The most frequently reported classes are Mirizzi types I (10.5–51%) and II (57%). There is a negligible prevalence of further forms of Mirizzi syndrome.2,3
Signs and symptoms of Mirizzi syndrome
Depending on the degree and location of the obstruction, signs and symptoms of Mirizzi syndrome can change. Common indications and symptoms include
- Obstructive jaundice (50-100%)
- Pain in the right upper quadrant or epigastric pain
- Fever and chills
- Nausea and vomiting
- Dark urine
- Tachycardia
- Anorexia
- Pale stools4
Management and treatment for mirizzi syndrome
Medical care and surgical treatment collaborate to manage and treat Mirizzi syndrome.
- Symptomatic management
The initial emphasis of treatment can be to reduce symptoms that include pain, nausea, and fever. Painkillers and anti-nausea drugs are administered to individuals to help them feel better.
- Surgical management
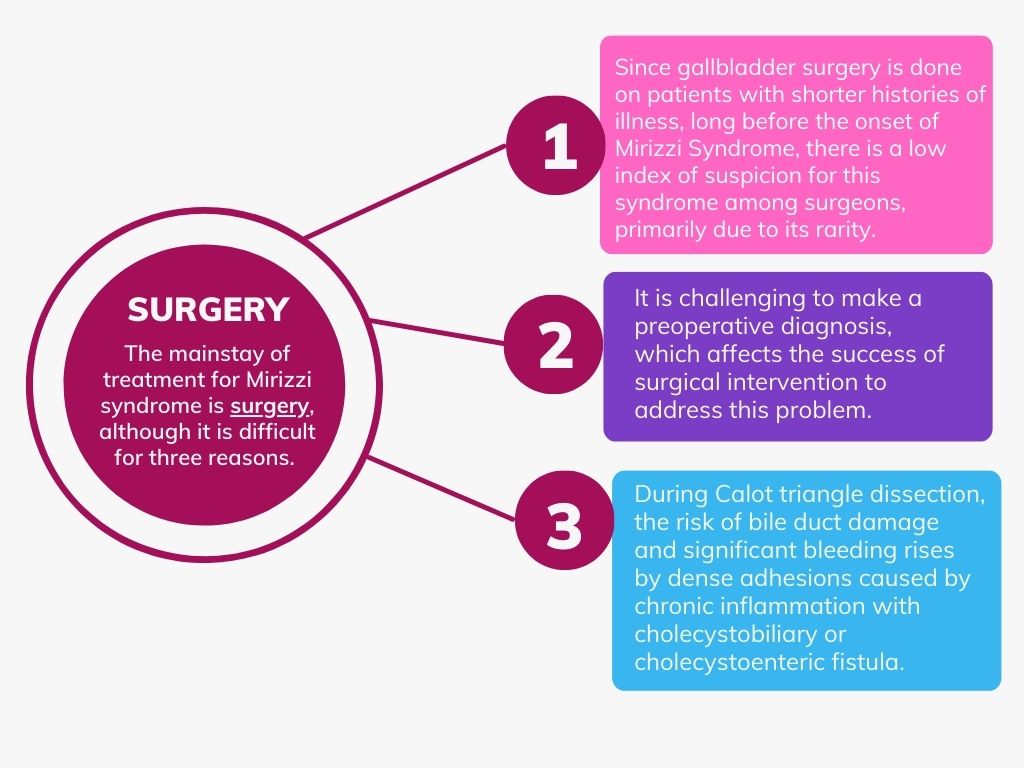
Created by: Deepika Rana
There are multiple surgical techniques, include
- Open surgical technique
Laparotomy is the preferred traditional procedure for treating Mirizzi Syndrome. It is primarily because laparoscopic surgery (smaller incisions) is less secure, has high conversion rates (between 31 and 100%) and has a higher risk of bile duct injury. Laparotomy has the advantage of improved sight, haptic feedback and gallbladder calculus removal before cholecystectomy despite its increased invasiveness, higher complication rate and prolonged postoperative hospital stay.
When Mirizzi Syndrome Type I does not involve a cholecystobiliary fistula, total cholecystectomy is an option. Retrograde fundus-first or partial (subtotal) cholecystectomy (PC or SC) occurs when significant inflammation prevents the safe dissection of the Calot triangle. When the quality of the tissue healing is questionable, it may be required to introduce a T-tube into the bile duct to decompress it and shape it to reduce the danger of bile leakage.
In Mirizzi Syndrome type II and type III, PC or SC can leave a cuff of the gallbladder or cystic duct utilised to repair the fistula of CBD (choledochoplasty). Choledocholenteric anastomosis is a recommended option for this approach.
- Preoperative biliary decompression
Le Roux et al. implemented preoperative draining with endoscopic stents or nasobiliary drain implantation by endoscopic retrograde cholangiopancreatography (ERCP) to avoid the insertion of T-tubes or abdominal drains while preventing postoperative problems. The Bile duct's intraoperative identification is made simpler by preoperative biliary drainage. The most effective surgical procedure for Type IV is generally agreed to be cholecystectomy and Roux-en-Y hepaticojejunostomy (RYHJ). However, other authors assert that Type III and Type IV fistulas with diameters greater than two-thirds of the CBD undergo treatment with RYHJ. Laparotomy is invariably the safest method of treating Mirizzi Syndrome Type V.
- Endoscopic techniques
Preoperative ERCP with sphincterotomy (dividing the sphincter) and nasal bile drainage (NBD insertion) is performed on patients with Mirizzi Syndrome Types I, II, and III, followed by laparoscopic subtotal cholecystectomy (LSC). NBD performs intraoperatively to decompress the bile duct, locate the CBD and carry out a cholangiography (to look at the structure of bile ducts and gallbladder). The remaining stones get extracted using mechanical lithotripsy, laser lithotripsy (LL), electrohydraulic lithotripsy (EHL) or chemical dissolution. The surgeons involved in these treatments must be highly skilled in endoscopy.
- Robot-assisted methods
Many authors have highlighted the value of robot-assisted approaches for treating Mirizzi Syndrome in recent years. Robot-aided methods, as opposed to laparoscopy, can offer improved visibility with a three-dimensional camera, and surgeons can do expert fine-tissue manipulation with endo wrist tools. The results of these procedures can be more effective when paired with endoscopic methods.
- Other new approaches
Laparoscopic trans-fistulous bile duct exploration, a recent procedure that combines LSC and infundi bulotomy to conduct EHL or LL for Type II, III, and IV patients, has been introduced by Chuang et al. Numerous other innovative procedures, such as single-operator peroral cholangioscopy, cystic duct balloon dilation at the intersection of the CBD and cystic duct stump for post-cholecystectomy Mirizzi Syndrome type I and double cannulation followed by a sphincterotomy and massive balloon dilation of the papilla, can provide a new direction in treatment strategy.5
Diagnosis
Clinical assessment, imaging tests, and occasionally invasive procedures serve to diagnose Mirizzi syndrome, mentioned in the picture below:
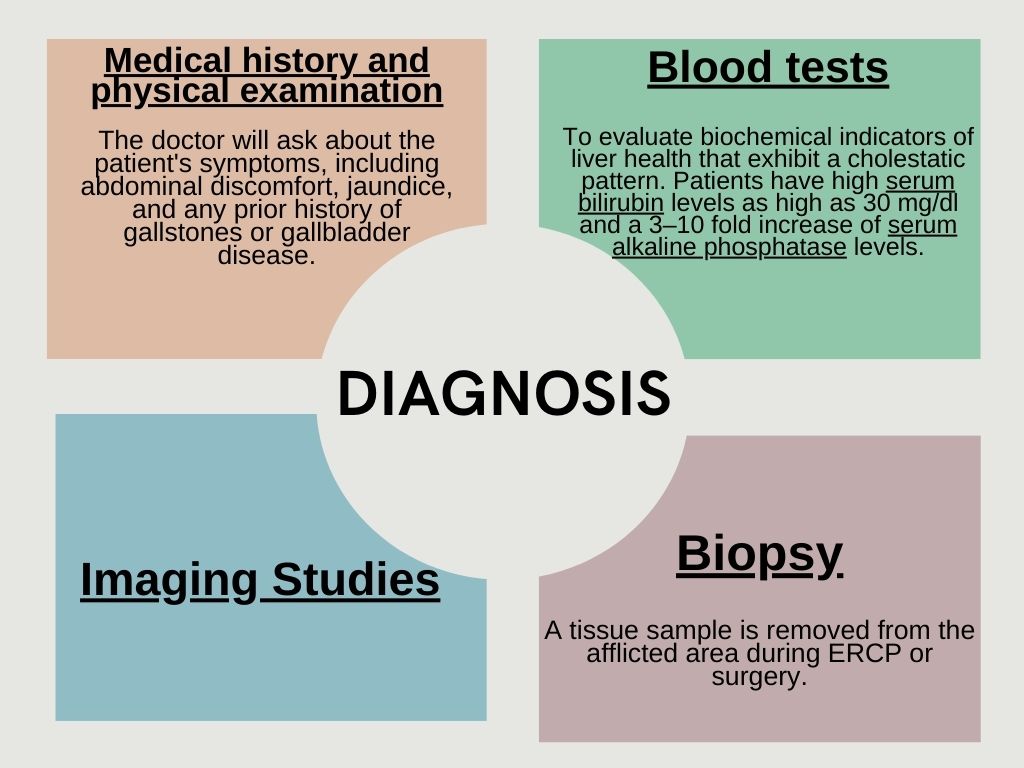
Serum bilirubin and alkaline phosphatase levels
Created By: Deepika Rana
Imaging studies
| Ultrasonography | Serves as a standard first step in the diagnosis of biliary disease while detecting cholecystitis, gallstones and signs of Mirizzi syndrome like a dilated CHD with a distal CBD or an oedematous gallbladder from acute cholecystitis. |
| Magnetic resonance cholangiopancreatography (MRCP) | A non-invasive imaging method to identify the usual symptoms of Mirizzi syndrome. When an ultrasound examination shows a dilated bile duct with signs of jaundice or bile duct stone impaction, MRCP confirmation is necessary. |
| ERCP | Given its high sensitivity (55% to 90%), ERCP classifies as the gold standard for determining the presence of the Mirizzi syndrome and is also a therapeutic method. |
| Computed Tomography (CT scan) | To get finer pictures of the gallbladder, bile ducts and surrounding tissues. |
| Nuclear imaging | Hepatobiliary iminodiacetic acid-diisopropyl iminodiacetic acid (HIDA-DISIDA) scintigraphy. A non-visualised gallbladder, a mild dilation of the CHD and delayed excretion into the duodenum are three sensitive and specific symptoms identified.3,6 |
FAQs
How can I prevent mirizzi syndrome?
Individuals can reduce their risk of developing Mirizzi syndrome by preventing gallstones, which usually result in the illness. Prevention measures comprise
- Healthy lifestyle: Obesity, diabetes mellitus, and insulin resistance are three components of the metabolic syndrome that influence the cause of cholesterol gallstones.
- Eating a balanced diet consisting of high-fibre and calcium lowers biliary hydrophobic bile acids and promotes regular gallbladder emptying.
- Exercise appears to prevent gallstone formation and reduce the incidence of symptomatic stones by roughly 30%.
- Staying Hydrated
- Avoiding smoking and limiting alcohol consumption.7
How common is mirizzi syndrome?
Mirizzi syndrome is uncommon. Only 0.1% of people with gallstones and 0.7% to 25% of individuals who underwent cholecystectomies will experience this syndrome. Although there may be a higher prevalence in elderly populations, there hasn't been a preference for either (AMAB) male or (AFAB) female patients with gallstones. An incidence rate for any particular ethnic group doesn't seem to exist.1
Is mirizzi syndrome fatal?
Mirizzi syndrome can cause serious problems, but with prompt diagnosis and proper care, it typically does not result in fatalities. The estimated percentage of mortality rates related to Mirizzi syndrome is between 5% and 31%.8
What can I expect if I have mirizzi syndrome?
The most typical manifestation is sudden, severe pain spreading from the right upper quadrant to the right shoulder. Nausea, vomiting, and a fever with chills are associated symptoms. Definitive therapy is required if gallstones start to cause symptoms and there are recurring episodes.9
When should I see a doctor?
A history of gallstones should be the first step in diagnosing and treating Mirizzi syndrome. If you experience repeated epigastric or right epigastric discomfort, mild to severe jaundice and fever, you should see a medical professional promptly.10
Summary
Due to the difficulty it presents with the unexpectedness of its onset, Mirizzi syndrome continues to be a fascinating area of research. Gallstones are prevalent, although it is uncommon. You can be carrying them without even realising it. Every attempt must be made to determine a preoperatively accurate diagnosis, conduct a precise and cautious operation to identify the kind of Mirizzi, and carry out the most appropriate course of therapy for each case.
References
- Jones MW, Ferguson T. Mirizzi syndrome. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Jul 17]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK482491/
- Beltrán MA. Mirizzi syndrome: History, current knowledge and proposal of a simplified classification. World J Gastroenterol [Internet]. 2012 Sep 14 [cited 2023 Jul 17];18(34):4639–50. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3442202/
- Mirizzi syndrome imaging: practice essentials, radiography, computed tomography. 2023 Apr 28 [cited 2023 Jul 19]; Available from: https://emedicine.medscape.com/article/370808-overview
- Valderrama-Treviño AI, Granados-Romero JJ, Espejel-Deloiza M, Chernitzky-Camaño J, Barrera Mera B, Estrada-Mata AG, et al. Updates in Mirizzi syndrome. Hepatobiliary Surg Nutr [Internet]. 2017 Jun [cited 2023 Jul 20];6(3):170–8. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5474450/
- Chen H, Siwo EA, Khu M, Tian Y. Current trends in the management of Mirizzi Syndrome. Medicine (Baltimore) [Internet]. 2018 Jan 26 [cited 2023 Jul 21];97(4):e9691. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5794376/
- Sanchez Garcia NL, Gordillo UP, Casas YH, Remedios IB, de la Torre RM, Sosa JR. Diagnosis and Treatment of Mirizzi Syndrome: Case Report and Literature Review. MedDocs Publishers; 2020 Nov 04 [cited 2023 Jul 24]; Annals of Gastroenterology and the Digestive System 2020; 3(1): 1026. Available from: https://meddocsonline.org/annals-of-gastroenterology-and-the-digestive-system/diagnosis-and-treatment-of-mirizzi-syndrome-case-report-and-literature-review.pdf
- Lammert F, Acalovschi M, Ercolani G, Erpecum KJ van, Gurusamy KS, Laarhoven CJ van, et al. EASL Clinical Practice Guidelines on the prevention, diagnosis and treatment of gallstones; European Association for the Study of the Liver (EASL) [Internet]. Elsevier; 2016 [cited 2023 Jul 24]. Journal of Hepatology 2016 vol. 65 j 146–181; Available from: https://www.journal-of-hepatology.eu/article/S0168-8278(16)30032-0/pdf
- Pak S, Valencia D, Sheehy B, Agbim U, Askaroglu Y, Dee C. Ticking bomb: asymptomatic mirizzi syndrome. Cureus [Internet]. [cited 2023 Jul 24];9(11):e1854. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5769986/
- Khokhar I, Adourian M, Delia E, Mohan G, Mathew M. Mirizzi syndrome: a case report and review of the literature. Cureus [Internet]. [cited 2023 Jul 24];14(4):e24375. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9126480/
- Zhou J, Xiao R, Yang J rui, Wang L, Wang J xing, Zhang Q, et al. Mirizzi syndrome complicated by common hepatic duct fistula and left hepatic atrophy: a case report. J Int Med Res [Internet]. 2018 Nov [cited 2023 Jul 24];46(11):4806–12. Available from: http://journals.sagepub.com/doi/10.1177/0300060518797246




