


Melanocytes are important cells found all over the body that produce melanin, the substance responsible for giving colour (or pigmentation) to hair, eyes and skin. However, when too many melanocytes are produced, excess cells can form masses or tumours, known as melanomas. Ocular melanoma refers to melanocyte cancer that occurs in the eye. It is considered an extremely rare form of melanoma, as it only affects around 7000 adults per year worldwide, with around 500-700 cases occurring in the UK.1 Although rare, ocular melanoma is the most common type of eye cancer found in adults - so it is important to know about the disease’s causes, symptoms, diagnosis and treatments, which will be discussed in this article.
Types of ocular melanoma
Ocular melanoma can be categorised into two main types. These types are based on where the tumour originates in the eye.
Uveal melanoma
80-90% of ocular melanomas originate from the part of the eye known as the uveal tract.2 These ocular melanomas are referred to as uveal melanomas.
The uveal tract is the pigmented middle layer of the human eye. As such, it is sandwiched between the outer layer, which consists of the transparent cornea and the white sclera, and the inner layer (or retina, which processes light that enters the eye and translates it into the images we see).3 The uveal tract itself is made up of 3 different parts, and melanocytes can be found in all of them:
- Choroid – the choroid is the largest part of the uveal tract. It is found directly behind the retina and covers the back of the eye. It holds the important function of supporting and nourishing the retina via its large network of blood vessels.4 Melanoma that develops in the choroid accounts for 90% of uveal melanomas.5
- Ciliary body – The ciliary body consists of approximately 5-6mm of muscle tissue that extends from the iris. This muscle contracts to help shape the part of the eye called the lens. The lens focuses light onto the retina at the back of the eye, helping you see. The ciliary body also produces a transparent fluid called aqueous humour, which maintains the correct pressure in the eye.4 Melanomas that develop in the ciliary body account for 6% of uveal melanomas.5
- Iris – the iris is the coloured part of the eye that you can see externally. It gives your eyes their blue, brown, or green colour and controls the amount of light which enters the eye by manipulating the size of the pupil.4 Only 4% of uveal melanomas develop in the iris.5
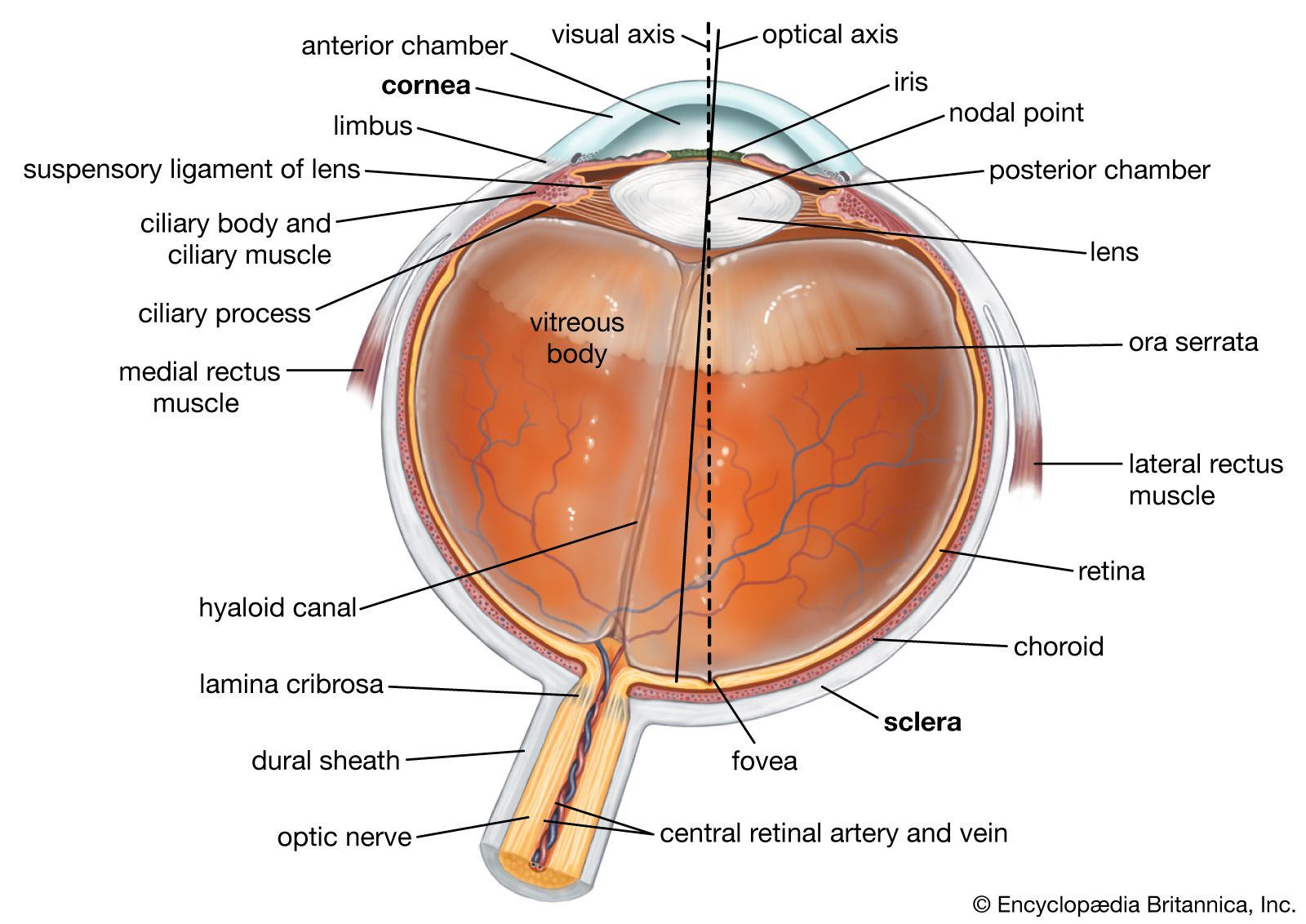
Figure 1. Anatomy of the eye with labelled parts (Encyclopedia Britannica).
Uveal melanoma is actually the most common eye cancer in adults in the Western world, with 5-7 people per 1 million developing this tumour throughout their life.2 If not caught early, uveal melanomas can spread to other organs within the body, such as the liver, lungs, and bones.6
Conjunctival melanoma
Around 5% of all ocular melanomas originate from melanocytes in the conjunctival epithelium - the layer of tissue covering the outer white sclera of the eye. The conjunctival epithelium is responsible for generating the moisture that covers the surface of the eye, which is crucial in helping the eyelids open and close.7 Tumours in this region of the eye are known as conjunctival melanomas.
Conjunctival melanoma is much rarer than uveal melanoma and only affects 1-2 people per 1 million in the Western world.8 Although rare, it is important that conjunctival melanoma is diagnosed early, as it becomes life-threatening if it spreads to other layers of the eye or the other parts of the body.7
Causes and risk factors
As with many cancer types, the exact underlying cause of ocular melanoma is unknown. However, multiple genetic and environmental factors are thought to play a role in the development of these tumours. There are different risk factors for the two categories of ocular melanoma:
| Risk Factor | Uveal Melanoma | Conjunctival melanoma |
| Genetic factors | Both uveal and conjunctival melanoma can be caused by changes or errors (mutations) in the DNA of melanocytes. DNA is the body’s genetic code and holds instructions to produce essential proteins and molecules which help cells, such as melanocytes, function properly. This includes proteins that control the life cycle, division, and death of cells. When errors occur within this code, the melanocytes may begin to replicate more quickly than normal, leading to the formation of tumours.9 Common mutations found in uveal melanoma differ from those found in conjunctival melanoma. Different mutations are associated with uveal and conjunctival melanoma: | |
- Mutations in the GNAQ and GNA11 genes (seen in 80-90% of patients)9 - Mutations in the BAP1 gene, particularly in patients who have a family history of uveal melanoma. BAP1 mutations are associated with larger tumours, an increased risk of metastasis (cancer spreading to other organs), and worse outcomes for patients.10 - Mutations in the SF3B1, PLCB4 and CYSLTR2 genes.8 | - Mutations in the BRAF gene (seen in 25-35% of patients).8 - Mutations in the TERT, NRAS, and NF1 genes.8 | |
| Exposure to ultraviolet radiation | Too much exposure to ultraviolet (UV) radiation, such as from the sun, can damage the DNA in melanocytes.11 This is particularly true for people with light eye and skin colour.12 Ultraviolet radiation exposure is a major risk factor for conjunctival melanoma, as the conjunctival epithelium is on the outer part of the eye and thus often exposed to direct sunlight.13 | |
| Age | - Most diagnosed patients are between ages 50 and 8014 - Melanoma of the iris is more common in younger patients (<20 years)14 | Most diagnosed patients are between ages 54 and 6715 |
| Sex | Biological sex has no influence on your risk of ocular melanoma.16 | |
| Nevi | A nevus (nevi for plural) is a growth or a mark that appears more pigmented or raised compared to the rest of an individual’s skin. Examples of nevi include freckles and birthmarks. Nevi can occur in the eye. Although most eye nevi are harmless, they may start growing and become an indicator of ocular melanoma.17 Below are examples of eye nevi conditions that can increase your risk of uveal and conjunctival melanoma: | |
| - Oculodermal melanocytosis (nevus of the Ota). This condition is congenital (present at birth) and is characterised by dark spots on/in the eye or surrounding areas. Individuals with oculodermal melanocytosis has a 1 in 400 chance of developing ocular melanoma over their lifetime.17 - Choroidal nevi - lesions at the back of the eye, which appear as bruises - Iris nevi – freckles/spots that appear in the white part of the eye | - Primary acquired melanosis - a condition characterised by the presence of brown spots of the conjunctival epithelium. Up to 75% of conjunctival melanoma patients first see their doctor with primary acquired melanosis18 | |
Signs and symptoms of ocular melanoma
You should see a doctor or ophthalmologist if you are experiencing any of the following symptoms:19
- Changes in the shape and/or size of the pupil
- Change in the position and movements of the eyeball
- Bulging eyes
- Dark spots growing on the iris
- Dark patches developing on the white part of the eye
- Flashing lights in vision
- Floaters (small black spots) in vision
- Vision problems, including blurry vision or losing part of your field of vision
- Irritation or pain in the eye
Whilst these symptoms may be due to less serious eye conditions (such as nevi), it is vital to see an ophthalmologist to rule out ocular melanoma.19 It is important to note that sometimes, people who have ocular melanoma do not show any signs of the disease until much later. As such, it is important to have routine eye exams to make sure your eyes are healthy.19
Diagnosis
If your ophthalmologist suspects you have ocular melanoma, they will use a series of more specific tests to reach a definite diagnosis. These tests include:20
- Eye ultrasound – this non-invasive imaging test uses high-frequency sound waves (from an instrument called a transducer) to take pictures of your eye
- Fluorescein angiography – this is another imaging test that involves injecting a dye into your arm. Pictures are taken as the dye passes through the blood vessels leading to the eye, revealing any abnormalities or blockages in the vessels supplying the eye with blood.
- Optical coherence tomography – this is a non-invasive imaging technique that uses light to take pictures of the uveal tract and the retina. These images can help diagnose uveal melanoma.
- Biopsy – if the above imaging tests are unable to provide an accurate diagnosis, your ophthalmologist may take a small sample of tissue from the surface of your eye for examination. This test is a lot more invasive than imaging tests, as it involves inserting a small needle into the eye.
If a doctor suspects the cancer may have already spread to other organs, further testing can take place, including:20
- Blood tests to assess liver function
- CT scans
- MRI scans
- PET scans
- Abdominal ultrasounds
Treatment options
There are several treatment options available for ocular melanoma patients, depending on the position of their tumour and how developed it is (i.e. whether the cancer has remained within the eye or has spread to other parts of the body).19 These include:
Surgical treatments:
- Surgery – One of the most common treatments for patients with early-stage and non-metastatic tumours. Surgery is used to remove the tumour and a small amount of surrounding tissue (to ensure complete removal).
- Enucleation – Enucleation can be used if the patient’s tumour is quite large and their vision can no longer be saved. This treatment involves removing the eye and part of the optic nerve (the nerve which carries messages from the brain to the eye) and replacing it with an artificial eye. The eyelids, eyelashes, eyebrows, and surrounding skin are not removed.
- Exenteration – If the tumour has compromised the patient’s vision and has spread to surrounding tissues, exenteration can be carried out. Extenteration involves removing the eye and optic nerve, as well as the muscles, nerves, and fat of the eye socket. After surgery, you will be fitted with an artificial eye and can undergo facial prosthetic surgery to replace lost tissue.
Radiation-based treatments:
Radiation is an energy source that is emitted as either particles or magnetic waves. It is commonly used for cancer therapies, as it can effectively kill cancer cells. Radiotherapies commonly used to treat ocular melanoma include:19
- Particle/proton beam radiotherapy – this treatment involves using invisible high-energy particles to target and kill cancer cells in the eye without affecting the surrounding healthy tissue.
- Brachytherapy – this treatment consists of ‘packaging’ radiation into small seeds or wires and placing them into the eye near the tumour. Brachytherapy is often used after surgery to ensure the cancer is completely eradicated.
- Plaque radiation therapy – plaque radiation therapy is similar to brachytherapy. However, rather than planting the radioactive seeds directly into the tumour, they are attached to a disk called a plaque. This plaque is placed on the outside wall of the eye to minimise damage to healthy tissue.
- Gamma knife radiosurgery – this treatment aims gamma rays (a type of high-energy radiation) directly at the tumour to kill cancer cells.
Other treatments
Other types of therapies available to ocular melanoma patients include.19
- Panretinal photocoagulation laser – this involves directing a laser at the blood vessels directly connected to the ocular melanoma, eventually starving the cancer cells of nutrients and killing them.
- Transpupillary thermotherapy – this involves using a laser to drastically raise the temperature of the tumour, making it too hot for cancer cells to survive.
- Cryotherapy – this involves periodically placing a very cold tool (called a freezing pen) onto the surface of the eye. The freezing and thawing of tumour cells helps prevent them from spreading.
Current clinical trials for future treatments
Despite the variety of treatments available for ocular melanoma patients, up to 50% of patients develop cancer elsewhere in the body. As a result, scientists are looking into new therapies that can be used to stop the spread of ocular melanoma and improve outcomes for patients. Here are some of the therapies that are currently being tested:21
- Immunotherapy – immunotherapy is a common type of cancer treatment that helps the patient’s immune system attack the cancer. As ocular melanomas often suppress the immune system, researchers hope that boosting the patient’s immune system will help slow tumour growth and kill cancer cells.
- Oncolytic viruses – this specific form of immunotherapy uses viruses to kill cancer cells by injecting them into tumours.
- Targeted therapy – as mentioned above, various genetic mutations are thought to encourage the development of ocular melanomas. Trials are currently attempting to reverse the effects of these mutations in the hopes of slowing tumour growth.
- Liver-directed therapy – up to 90% of patients with advanced uveal melanoma develop cancer in the liver.21 As such, many trials are focused on preventing or treating liver cancer.
Summary
Ocular melanoma is the most common type of eye cancer in adults and affects melanocytes, the cells that give colour to our eyes, hair and skin. There are several genetic and environmental risk factors that can lead to the development of ocular melanoma, such as exposure to UV radiation. The disease usually presents as dark spots in the eye and ultimately leads to vision problems. Although there are various treatments for ocular melanoma, there is no cure, and the cancer can often spread to other organs in the body. However, current clinical trials are being undertaken to address this issue and to improve the quality of life of ocular melanoma patients.
FAQs
How can I prevent ocular melanoma?
It’s important to protect yourself from ultraviolet radiation. This involves wearing sunscreen, sunglasses, and wide hats in bright sunlight. Further, regular eye examinations are essential for the early detection of ocular melanoma and avoidance of more serious symptoms.
How serious is ocular melanoma?
Small ocular melanomas may not cause any symptoms, but they can cause vision problems if they occur in a critical part of the eye. However, if they are caught early, ocular melanomas can be treated with surgery, radiation, or other treatments.
Very advanced ocular melanomas, however, can cause serious symptoms, including complete vision loss, and can be fatal if they spread to other organs.
What is the survival rate for ocular melanoma?
Depending on the severity of the melanoma (i.e. if and how much it has spread to other parts of the body), the survival rate can vary. The 5-year survival rate for patients where cancer remains within the eye is roughly 85%; the 5-year survival rate for patients whose cancer has spread to the surrounding tissues is roughly 65%; and the 5-year survival rate for patients whose cancer has spread to distant organs (such as the liver) is 15%.22
Can ocular melanoma come back?
Unfortunately, ocular melanoma can recur after treatment. As such, it is important to have checkups every 6-12 months in order to check for recurrence.
References
- Helgadottir H, Höiom V. The genetics of uveal melanoma: current insights. Appl Clin Genet. 2016;9:147–55.
- Kaliki S, Shields CL. Uveal melanoma: relatively rare but deadly cancer. Eye. 2017;31(2):241–57.
- Maggs DJ, Miller PE, Ofri R. Slatter’s Fundamentals of Veterinary Ophthalmology. 6th ed. Elsevier: St. Louis, Missouri, 2018.
- Photobiology of the uveal tract [Internet]. Accessed Sep 13 2023 via: http://photobiology.info/Hu.html
- Shields CL, Furuta M, Thangappan A, Nagori S, Mashayekhi A, Lally DR, et al. Metastasis of uveal melanoma millimeter-by-millimeter in 8033 consecutive eyes. Arch. Ophthalmol. 2009;127:989–98.
- Collaborative Ocular Melanoma Study Group. Assessment of metastatic disease status at death in 435 patients with large choroidal melanoma in the Collaborative Ocular Melanoma Study (Coms): COMS report no. 15. Arch. Ophthalmol. 2001;119:670–6.
- Wong JR, Nanji AA, Galor A, Karp CL. Management of conjunctival malignant melanoma: a review and update. Expert Rev Ophthalmol. 2014;9:185–204.
- van Poppelen NM, de Bruyn DP, Bicer T, Verdijk R, Naus N, Mensink H, et al. Genetics of ocular melanoma: insights into genetics, inheritance and testing. Int. J. Mol. Sci. 2021;22(1):336.
- Silva-Rodríguez P, Fernández-Díaz D, Bande M, Pardo M, Loidi L, Blanco-Teijeiro MJ. Gnaq and gna11 genes: a comprehensive review on oncogenesis, prognosis and therapeutic opportunities in uveal melanoma. Cancers. 2022;14:3066.
- Uner OE, See TRO, Szalai E, Grossniklaus HE, Stålhammar G. Estimation of the timing of BAP1 mutation in uveal melanoma progression. Sci Rep. 2021;11:8923.
- National Institutes of Health. How UV radiation triggers melanoma [Internet]. Last updated Feb 7 2011, accessed Sep 13 2023 via https://www.nih.gov/news-events/nih-research-matters/how-uv-radiation-triggers-melanoma
- Weis E, Shah CP, Lajous M, Shields JA, Shields CL. The association between host susceptibility factors and uveal melanoma: a meta-analysis. Arch Ophthalmol. 2006;124:54–60.
- Chang E, Demirci H, Demirci FY. Genetic aspects of conjunctival melanoma: a review. Genes. 2023;14:1668.
- McLaughlin CC, Wu XC, Jemal A, Martin HJ, Roche LM, Chen VW. Incidence of noncutaneous melanomas in the U.S. Cancer. 2005;103:1000–7.
- Jain P, Finger PT, Fili M, Damato B, Coupland SE, Heimann H, et al. Conjunctival melanoma treatment outcomes in 288 patients: a multicentre international data-sharing study. Br. J. Opthalmol. 2021;105:1358–64.
- Stålhammar G. Sex‐based differences in early and late uveal melanoma‐related mortality. Cancer Med. 2022;12:6700–10.
- Chan HHL, Kono T. Nevus of Ota: clinical aspects and management. Skinmed. 2003;2:89–96.
- Shields JA, Shields CL, Mashayekhi A, Marr BP, Benavides R, Thangappan A, et al. Primary acquired melanosis of the conjunctiva: experience with 311 eyes. Trans Am Ophthalmol Soc. 2007;105:61–72.
- Jovanovic P, Mihajlovic M, Djordjevic-Jocic J, Vlajkovic S, Cekic S, Stefanovic V. Ocular melanoma: an overview of the current status. Int J Clin Exp Pathol. 2013;6:1230–44.
- Patel DR, Patel BC. Ocular melanoma. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023. Last updated May 24 2023, accessed Sep 13 2023 via: http://www.ncbi.nlm.nih.gov/books/NBK551647/
- Sussman TA, Funchain P, Singh A. Clinical trials in metastatic uveal melanoma: current status. Ocul. Oncol. Pathol. 2020;6:381–7.
- Cancer.Net. Eye melanoma - statistics [Internet]. Last updated Feb 2012, accessed Sep 13 2023 via: https://www.cancer.net/cancer-types/eye-melanoma/statistics




