


Introduction
Schistosomiasis, one of the most neglected tropical diseases, is a parasitic disease (blood flukes), which is also known as bilharzia or snail fever. It is found in 78 countries in contaminated water.1
Schistosomiasis is caused by a parasite that targets several organs, including the intestine, liver, bladder, and urethra.1 The World Health Organisation (WHO) has estimated that around 251.4 million people in 2021 required treatment to prevent this parasitic disease. Table 1 illustrates the different species that cause schistosomiasis and the region of prevalence. Annually, schistosomiasis kills 280,000 people, and 779 million people are at risk of contracting the infection. Despite this, schistosomiasis is a neglected tropical disease due to many factors. One example is that schistosomiasis is situated primarily in sub-Saharan Africa, in poor communities, and there is a lack of concern by politicians, which leads to failure to initiate national strategic plans.3 Since it is prevalent in areas of high poverty and underdevelopment, the exposure to infection is higher where water sources are unsafe.4
Table 1. The species that are known to infect humans (the most common are highlighted in bold) and their regions of prevalence.2
| Species | Region |
| S. haematobium | Africa and Middle East |
| S. intercalatium | Central Africa |
| S. japonica | China, Southeast Asia |
| S. mansoni | Africa, Middle East and South America |
| Africa and the Middle East | Lao, People’s Democratic Republic and Cambodia |
Epidemiology
The most prevalent form of schistosomiasis is the chronic form, which causes urogenital disease. The average age of infection is 2 years old. Areas like Kenya have an average age of initial infection of 5 to 14 years old.5 As shown in Table 1, S. japonicium is prevalent in China. This species causes the most deadly disease out of the major Schistosoma, as some researchers speculate that the female worms release a higher yield of eggs, and the adult worm also has the longest lifespan in contrast to the other species, causing schistosomiasis.6 S. japonicium was first recorded in 1905, and the mortality rate was initially high due to a lack of prevention and control of the disease. However, by 1949, the Chinese government had implemented a national control programme, decreasing its incidence.
Historical background
Theodor Maximilian Bilharz, a German physician, and Patrick Manson, known as the ‘father of tropical medicine’, provided knowledge of parasites and their evolution with humans. Their discovery of causative agents was a remarkable point in parasitic research. The word ‘schistosomiasis’ is derived from the Greek language; ‘schistos’ means ‘to split’, and ‘soma’ means ‘body’. In 1852, the two pathologists observed embryos from the schistosomiasis eggs in the bladder and their passage in urine to fresh water and concluded that there was a link between the parasite and hematuria (blood in the urine). In the late 19th century, the life cycle of schistosomiasis was observed by Robert Thomson Leiper in aquatic snails.7
The life cycle of schistosomiasis and transmission
Figure 1 shows the life cycle of the chistosoma parasite. When the cercariae (larvae) enter the portal blood of the liver, the effects slightly differ depending on the species. The adult Schistosoma parasites are found to be 1 to 3 cm long. Adult S. intercalatum, S. mekongi and S. japonicium remain in the portal and mesenteric vessels. This differs for S. haematobium, which migrates to the vesical plexus.8 Here, they mature into adults and begin to release eggs. An immune reaction will occur in response to the infection by Schistosoma. However, the immune cells cannot kill the eggs, resulting in liver granuloma.9 For transmission to occur, a combination of events need to happen: firstly, the presence of contaminated water, particularly with faeces or urine containing Schistosoma eggs. Secondly, there is the presence of the freshwater snail, which is the intermediate host, and thirdly, there is human contact with the host snail.10
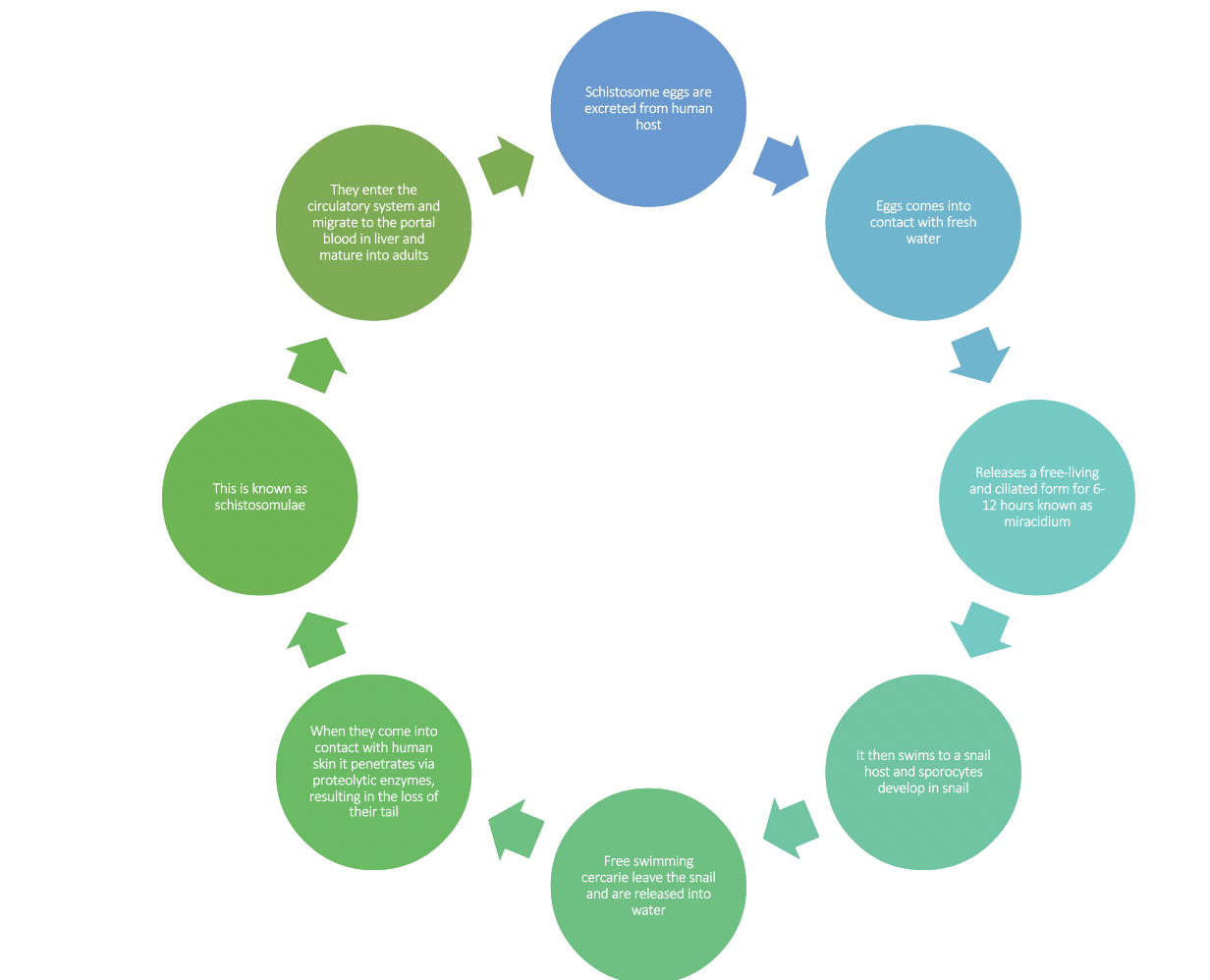
Figure 1: The summarised life cycle of schistosomiasis.8 This life cycle is dependent on an intermediate host to infect humans.
Clinical presentation
The clinical presentation of schistosomiasis consists of three phases: acute, chronic, and advanced. In acute schistosomiasis, the schistosome eggs go into host tissues. The symptoms at this stage include abdominal pain, blood in the stools or urine, fatigue, and fever. This stage is common in people who travel to areas where schistosomiasis is endemic. During the chronic and advanced stages, the schistosome eggs can trigger an inflammatory response in the urinary system when the eggs are present in the host tissues. When the eggs induce an inflammatory response this leads to complications, for example, the eggs will instigate hyperplasia (increased cell production) and polypolis (the formation of polyps (growths) in the colon). S. japonicium and S. mansoni target the liver.10
Immediate phase: 2–3 days:
- Red, itchy rash on skin
Acute phase: 2–12 weeks:
- Abdominal pain, diarrhoea, blood in stool (intestinal manifestation)
- Fever
- Muscle and joint pain
- Cough and chest pain
- Blood in the urine (urogenital manifestation)
- Genital lesions, vaginal bleeding and nodules in the vulva (in those assigned female at birth)
Chronic phase: 2–5 years:
- Anaemia
- Enlarged liver and occasionally spleen
- Bladder, kidney and prostate cancer
- Liver and kidney failure
- Lung damage, persistent cough, shortness of breath
- Brain damage resulting in seizures, weakness and numbness
- In children: anaemia, stunting, reduced cognitive ability
Diagnosis and detection
There are several detection methods used to identify schistosomiasis. These include microscopy tests on urine and stools, antibody detection methods, and DNA detection. For urine and stool detection, the Kato-Katz (KK) test examines a faecal smear to identify whether there are eggs present. This detection tool is cheap and straightforward to use; therefore, it is used in poorer areas. However, it does lack sensitivity.13 ELISA (enzyme-linked immunosorbent assay) is a common tool used to detect antibodies. It has greater sensitivity; however, false positives can occur. Additionally, antibody detection cannot distinguish between Schistosoma species, which can be a disadvantage.14 DNA detection assays are also used to detect schistosomiasis. This involves PCR (polymerase chain reaction), which detects eggs in urine, faeces or saliva. It has the best specificity and sensitivity out of the three, but this means that it is also very expensive, which may not be an available option in developing nations.12 It is important to provide cheap diagnostic tools in developing nations for them to be accessible to those who urgently need them.
Prevention and control
The main strategy for preventing schistosomiasis is avoiding freshwater lakes and rivers. This includes swimming or any other activity. However, if the water is indeed infected, it is vital to do vigorous towel drying to prevent the cercariae from penetrating the skin via mechanical penetration. Additionally, it is recommended by the WHO that preventative chemotherapy be used to control the incidence of infection.8
Treatment and management
Currently, the only treatment available for schistosomiasis is praziquantel, which is a drug used for mass drug administration (MDA). The dosage recommended is 40mg/kg as a single dose. This treatment is also safe for pregnant women. Despite being an effective treatment, it has no efficacy against eggs and immature worms.15
Summary
Schistosomiasis is a neglected tropical disease that is overlooked due to socioeconomic factors. Schistosomiasis can cause chronic illness if left untreated. It is prevalent in many areas, and it is vital to make sure that you are aware of the consequences of drinking or swimming in fresh water in these areas. The infection is common at a young age, and it can become deadly in the case of S. japonicium. Fortunately, the use of praziquantel, the primary drug used to tackle the disease, is effective. However, a disadvantage to this drug is that it does not effectively target immature worms. Despite these challenges, research on treatment and management continues to fight against schistosomiasis, as it remains an outstanding global health concern.
FAQs
What is the main cause of schistosomiasis?
The main cause of schistosomiasis is people who contact with water contaminated with a parasitic worm.
What happens if you have schistosomiasis?
You may experience abdominal pain, diarrhoea, swelling and blood in your urine or stool. You may also experience pain and numbness in your legs when excreting urine.
Can schistosomiasis go away on its own?
It can be treated with praziquantel.
Is schistosomiasis caused by a tapeworm?
No. It is caused by trematode worms known as flukes.
References
- Viana M, Faust CL, Haydon DT, Webster JP, Lamberton PHL. The effects of subcurative praziquantel treatment on life-history traits and trade-offs in drug-resistant Schistosoma mansoni. Evol Appl. 2018 Apr.11(4):488–500.
- Vale N, Gouveia MJ, Rinaldi G, Brindley PJ, Gärtner F, Correia Da Costa JM. Praziquantel for schistosomiasis: single-drug metabolism revisited, mode of action, and resistance. Antimicrob Agents Chemother [Internet]. 2017 May [cited 2023 Oct 20].61(5):e02582–16. Available from: https://journals.asm.org/doi/10.1128/AAC.02582-16
- Utzinger J, Raso G, Brooker S, De Savigny D, Tanner M, Ørnbjerg N, et al. Schistosomiasis and neglected tropical diseases: towards integrated and sustainable control and a word of caution. Parasitology [Internet]. 2009 Nov [cited 2023 Oct 20].136(13):1859–74. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2791839/
- King CH. Schistosomiasis: challenges and opportunities. The causes and impacts of neglected tropical and zoonotic diseases: Opportunities for integrated intervention strategies [Internet]. National Academies Press (US); 2011 [cited 2023 Oct 20]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK62510/
- Lackey EK, Horrall S. Schistosomiasis. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Oct 20]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK554434/
- Chen M. Assessment of morbidity due to Schistosoma japonicum infection in China. Infect Dis Poverty [Internet]. 2014 Feb 14 [cited 2023 Oct 20].3:6. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3928580/
- Di Bella S, Riccardi N, Giacobbe DR, Luzzati R. History of schistosomiasis (Bilharziasis) in humans: from Egyptian medical papyri to molecular biology on mummies. Pathog Glob Health [Internet]. 2018 Jul [cited 2023 Oct 20].112(5):268–73. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6225400/
- Inobaya MT, Olveda RM, Chau TN, Olveda DU, Ross AG. Prevention and control of schistosomiasis: a current perspective. Res Rep Trop Med [Internet]. 2014 Oct 17 [cited 2023 Oct 20.5:65–75. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4231879/
- JENKINS SJ, HEWITSON JP, JENKINS GR, MOUNTFORD AP. Modulation of the host’s immune response by schistosome larvae. Parasite Immunol [Internet]. 2005 [cited 2023 Oct 20].27(10–11):385–93. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1825761/
- Gray DJ, Ross AG, Li YS, McManus DP. Diagnosis and management of schistosomiasis. BMJ [Internet]. 2011 May 17 [cited 2023 Oct 20].342:d2651. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3230106/
- Carbonell C, Rodríguez-Alonso B, López-Bernús A, Almeida H, Galindo-Pérez I, Velasco-Tirado V, et al. Clinical spectrum of schistosomiasis: an update. J Clin Med [Internet]. 2021 Nov 25 [cited 2023 Oct 20].10(23):5521. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8672275/
- Ajibola O, Gulumbe BH, Eze AA, Obishakin E. Tools for detection of schistosomiasis in resource limited settings. Med Sci (Basel) [Internet]. 2018 May 23 [cited 2023 Oct 20].6(2):39. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6024580/
- Weerakoon KGAD, Gobert GN, Cai P, McManus DP. Advances in the diagnosis of human schistosomiasis. Clin Microbiol Rev [Internet]. 2015 Oct [cited 2023 Oct 20].28(4):939–67. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4548261/
- Mahmoud AAF. Schistosomiasis. World Scientific; 2001. p526.
- Hailegebriel T, Nibret E, Munshea A. Efficacy of praziquantel for the treatment of human schistosomiasis in Ethiopia: a systematic review and meta-analysis. J Trop Med [Internet]. 2021 Dec 20 [cited 2023 Oct 20].2021:2625255. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8712180/




