


Introduction
As per statistics, 3% of births are twins, and it is observed that non-identical (dizygotic) twins are seen more frequently than identical (monozygotic).1 The global prevalence of monozygotic twins worldwide is approximately seen to be 3 to 5 per 1000 childbirths.1 Despite such little prevalence, numerous complications occur. An interesting and rare complication is the Twin-To-Twin Transfusion Syndrome (TTTS).
What is twin-to-twin transfusion syndrome?
In simple terms, TTTS is a condition where there is a flow or transfusion of blood from one twin to the other inside the womb.2 The blood is responsible for carrying nutrients and oxygen to the baby and, in return, carries waste materials out of the body to the placenta. Due to the sharing of blood vessels among the twins, this process becomes unbalanced, and one fetus turns out to be significantly different from the other, both physically and physiologically.2
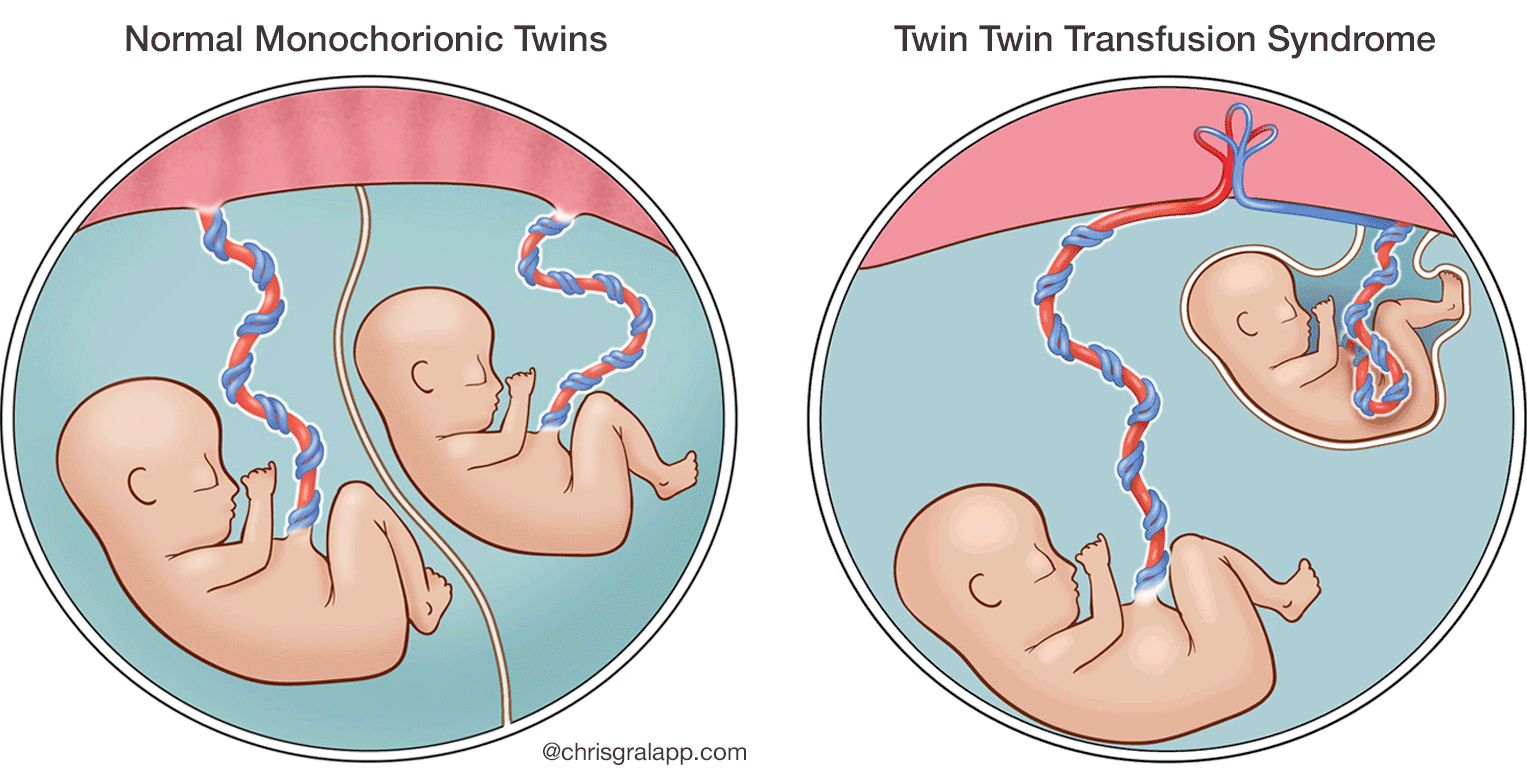
Fig1 Shows the difference in the structure of the fetus for a normal twin vs a TTTS twin.
Normal structure of the womb
Normally, the womb of a pregnant person carrying two or more foetuses has one placenta, one amniotic sac and two umbilical cords or two placentas, two amniotic sacs and two umbilical cords or one placenta, two sacs and two umbilical cords as shown in the figure.3 The primary function of the placenta is to provide oxygen and nutrients to the baby, and it does so by forming blood vessels around the umbilical cord. This ensures that a sufficient amount of blood is exchanged via the placenta. The amniotic sac gives enough space for the fetus to grow equally, protects it from exterior shocks and regulates the body temperature.4
Use of placenta in monozygotic (MZ) vs dizygotic (DZ) twins
As mentioned above, the main function of the placenta is to supply blood vessels and carry oxygen and nutrients. In MZ twins, as there is one placenta, there may be an unequal distribution of blood vessels seen among the fetuses. This means that one fetus might get more while the other might end up getting less. In some cases, the blood vessels join together in the twins, which causes a transfusion of blood from one fetus to another, as shown in Figure 1 and this gives rise to TTTS.3
In DZ twins, this generally is not seen because they are fertilized from two different eggs, meaning that the babies do not share a placenta.5
What happens in TTTS?
In TTTS, the blood volumes are substantially different and can result in abnormal or rather different rates of growth in the babies. This can mean different rates of development and can rarely be fatal.
Occurrence of TTTS worldwide
As per the literature, 70% of identical twins (MZ twins) are seen to share a placenta, and among them, 10-15% of babies are seen to be affected by TTTS.1 That means it is more common in MZ twins than DZ twins.
Causes and risk factors
Although there is no exact reason for the cause of this rare syndrome, some of the most postulated causes are explained below.
Direct connections between smaller arteries and veins
Also called the placental anastomoses. The exact reason as to why this happens is unknown. If the net blood flow during these direct connections remains the same, the babies can develop as normal. However, if an imbalance occurs, it can lead to complications.3 During such cases, the twin who received more blood is termed as a recipient while the other is called a donor.3 What happens to these babies physiologically is discussed below.
Placental abnormalities
A very interesting study conducted by Wang et al. studied about 48 placentas of TTTS from 2014 to 2019 and found a positive correlation between the placenta and the pregnancy age. The study concluded that the area on the placenta where the umbilical cord attaches plays a crucial role. It must ideally be attached to the centre of the placenta; if attached on the side, it may lead to TTTS.6
Monochorionic-monoamniotic twins
This means twins who share one placenta and one amniotic sack, which is very rare, have a greater risk of developing blood vessel connections leading to TTTS.1
Maternal factors
Age can be a risk factor, but there is no strong evidence confirming the same, as there have been reports of TTTS in pregnant people belonging to various age groups.
Genetic predisposition
Some literature suggests thrombophilia gene inherited from the mother can lead to TTTS, but it cannot be said for certain as the study was performed on less number of subjects.7
Effect of TTTS on the child
As per an article by Borse, as one baby receives less blood, there is evidence of comparatively smaller organs, especially kidneys, due to lower volumes of blood. This also affects the child's urine production ability.8
The recipient twin, due to more fluid volume, tends to grow faster and develops a larger bladder. They also are at risk of cardiac stretch and other heart-related problems and try to maintain homeostasis by excreting excess fluid into the amniotic fluid.8
Signs and symptoms
Diagnostic ultrasound findings
This is the primary mode of diagnosis of early signs of TTTS. Discordant (unequal) growth, Amniotic fluid level imbalances, small or no urinary bladder of the donor fetus, swelling of the recipient fetus or fetal death are some of the most common signs seen during the ultrasound.6
Maternal sensations
Common signs seen by the pregnant person are abdominal pain, sudden weight gain and swelling. Around 18 weeks of pregnancy is when the pregnant person can notice an initial symptom of TTTS.9
Staging the severity of TTTS
Although TTTS might be present, understanding the severity is crucial to decide the appropriate treatment option. As per the Quintero staging system, there are 5 stages of increasing the severity of TTTS.9
- Stage 1 is where the is a distinct imbalance of fluid seen between the donor and the recipient. This confirms the presence of TTTS. Generally, when one sac is less than 2cm and the other more than 8cm, an imbalance is considered.
- Stage 2 is when the bladder stops to be visible for the donor twin during ultrasound screening.
- Stage 3 is confirmed when there is an abnormal Doppler velocimetry seen in the foetus.
- Stage 4 is when significant swelling can be seen in the foetus. In this case, the recipient foetus.
- Stage 5 is when either one or both foetuses have passed away
Although the above staging system is well established and has proven useful, the complications progress quickly to the next stage and therefore it is always recommended to have check-ups at least twice a week to avoid further complications.10
Complications
Fetal complications
If not managed quickly, there can be some serious complications like Fetal growth restriction, fetal loss, miscarriage, and delivery before the due date – such babies have an additional risk of complications like cerebral palsy.11 If the baby is born, the recipient twin is at a high risk of developing cardiac dysfunction, certain brain abnormalities and growth restriction in either twin.11
Maternal complications
The most commonly seen complications to the pregnant person are Preterm labour, Preeclampsia (increased blood pressure), psychological trauma etc.
Treatment Options:
Pregnant people should have regular check-ups, especially if the twins are sharing one placenta and look out for early signs of TTTS right from 15-22 weeks of pregnancy.11
Intrauterine procedures like Amino drainage are used to reduce the fluid, especially from the recipient twin. This reduces the pressure and increases blood flow towards the donor twin. Laser ablation therapy – where the heat of the laser beam blocks some of the shared vessels, which then ensures equal blood flow to both twins.11
Immediate and correct management options will help save the child, but if left untreated, it could lead to fetal death.
If TTTS is presented acutely, C C-section would be the most viable option to save the babies on time. In cases with less severity, vaginal mode can be considered. Once the baby is born, it will be monitored closely for a few days before getting a discharge.
Summary
In conclusion, TTTS is a rare condition seen in multiple pregnancies. It is more common when the twins share one placenta and one or two amniotic sacs. Due to a single placenta being used, the blood vessels tend to form connections between small arteries and veins, leading to transfusion of blood and fluid from one twin to the other. The attachment of the umbilical cord to the placenta also plays an important role in determining the consequence leading to TTTS. Ultrasonography is the only initial way of determining this condition. Early detection is possible right from 15 weeks of pregnancy. Generally, one child looks enlarged and the other small. The pregnant person can experience sudden weight gain and severe pain. Choosing the right treatment option is crucial. For serious cases, an emergency C-section must be performed. If left untreated, it can lead to death of the foetus in most cases. Therefore, it is vital to understand the importance of early diagnosis and intervention.
FAQs
- Will all pregnant people with one placenta and 2 babies develop TTTS?
No. It is not always the case, but such cases are at the highest risk of developing TTTS. However, by timely checkups, early diagnosis can be made.
- Is the C-section the only option for pregnant people diagnosed with TTTS?
Not necessarily. In acute cases of TTTS, C-section can be the most reliable solution but vaginal deliveries have also occurred with pregnant people diagnosed with TTTS.
- Are the babies healthy after birth?
While it is most likely that the babies will be healthy after birth, if they are not treated on time, the children may develop some neurological conditions.
References
- Miller JL. Twin-to-twin transfusion syndrome. Transl Pediatr [Internet]. 2021 May [cited 2023 Oct 3];10(5):1518–29. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8193008/
- Agrawal P, Vaidya A, Vaidya A, Phuyal S, Pandey A. Twin to twin transfusion syndrome: a case report. JNMA J Nepal Med Assoc [Internet]. 2022 Dec [cited 2023 Oct 3];60(256):1056–8. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9795135/
- Marceau K, McMaster MTB, Smith TF, Daams JG, van Beijsterveldt CEM, Boomsma DI, et al. The prenatal environment in twin studies: a review on chorionicity. Behav Genet [Internet]. 2016 [cited 2023 Oct 4];46:286–303. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4858569/
- Shamsnajafabadi H, Soheili ZS. Amniotic fluid characteristics and its application in stem cell therapy: A review. Int J Reprod Biomed [Internet]. 2022 Sep 6 [cited 2023 Oct 4];20(8):627–43. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9596929/
- Machin GA, Bamforth F. Zygosity and placental anatomy in 15 consecutive sets of spontaneously conceived triplets. Am J Med Genet [Internet]. 1996 Jan 22 [cited 2023 Oct 4];61(3):247–52. Available from: https://onlinelibrary.wiley.com/doi/10.1002/(SICI)1096-8628(19960122)61:3<247::AID-AJMG8>3.0.CO;2-R
- Wang X, Shi H, Li L, Yuan P, Zhao Y, Wei Y. Study of the placental characteristics and time of onset of twin-to-twin transfusion syndrome. Placenta [Internet]. 2021 Jan 1 [cited 2023 Oct 5];103:10–5. Available from: https://www.sciencedirect.com/science/article/pii/S0143400420304069
- Giannubilo SR, Fiorelli A, Marzioni D, Tossetta G, Capogrosso G, Ciavattini A. Maternal inherited thrombophilia in monochorionic twin pregnancy with twin-twin transfusion syndrome. J Clin Med [Internet]. 2022 Nov 29 [cited 2023 Oct 5];11(23):7054. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9736336/
- Borse V, Shanks AL. Twin-to-twin transfusion syndrome. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Oct 5]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK563133/
- Bamberg C, Hecher K. Twin-to-twin transfusion syndrome: Controversies in the diagnosis and management. Best Practice & Research Clinical Obstetrics & Gynaecology [Internet]. 2022 Nov 1 [cited 2023 Oct 6];84:143–54. Available from: https://www.sciencedirect.com/science/article/pii/S1521693422000529
- Simpson LL. Twin-twin transfusion syndrome. American Journal of Obstetrics and Gynecology [Internet]. 2013 Jan 1 [cited 2023 Oct 5];208(1):3–18. Available from: https://www.sciencedirect.com/science/article/pii/S0002937812019801
- Rao A, Sairam S, Shehata H. Obstetric complications of twin pregnancies. Best Practice & Research Clinical Obstetrics & Gynaecology [Internet]. 2004 Aug 1 [cited 2023 Oct 6];18(4):557–76. Available from: https://www.sciencedirect.com/science/article/pii/S1521693404000501




