


Vestibulodynia is a condition defined by chronic pain or discomfort occurring in the outer opening of the vulva, which is also known as the vestibular region.1 Vestibulodynia is a subset of vulvodynia (persistent pain in the vulva).2 Despite it being a common condition, it is extremely underdiagnosed.3 Approximately 50% of GPs in northern England have reported at least 1 patient a month with vulval pain,4 and studies have observed at least 6% prevalence in people assigned female at birth (AFAB) of all ages and ethnicities. Vestibulodynia and vulvodynia prevalence is likely to be higher due to misdiagnosis, as it is usually mistaken for thrush or vaginismus.5 To understand vestibulodynia, it is important to have a brief understanding of vulvar anatomy. The vulva encompasses the external area of the female genitalia. The vestibule is the area of tissue that surrounds the entrance of the vagina and is enclosed by the labia minora.6 Vulvodynia is an umbrella term to define chronic pain in the vulva region, whereas vestibulodynia is pain localised to the vestibule.
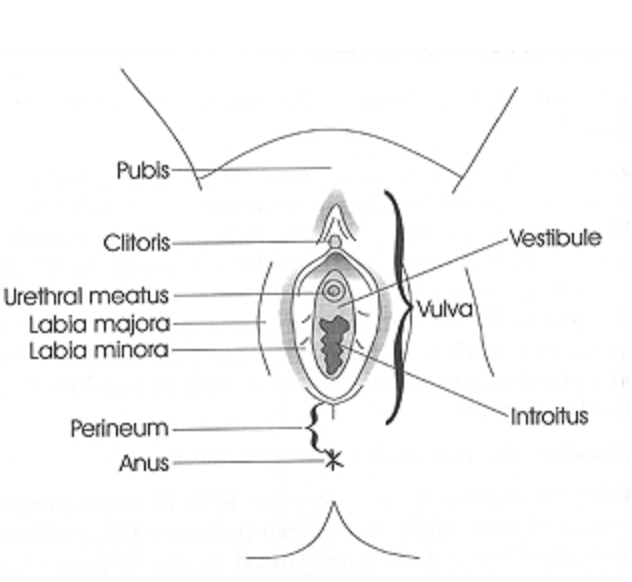
Diagram reproduced with permission from The Interstitial Cystitis Survival Guide by Robert Moldwin, MD, New Harbinger Publications, Inc. © 2000.
Symptoms
The primary symptoms of vestibulodynia include hypersensitivity to touch, burning or stinging sensations, redness and inflammation. However, it is important to note that the degree of pain can vary between individuals; for instance, some people experience pain but can tolerate penetrative sex, whilst others experience extreme discomfort in response to light touch caused by tight clothing.4
Diagnostic criteria
Vestibulodynia is difficult to diagnose and is often misdiagnosed. Diagnosis is dependent on physical examination of the vestibule, with the diagnostic criteria including hypersensitivity to light touch, visible inflammation and redness. However, the absence of these characteristics is common in some cases of vestibulodynia, resulting in underdiagnosis. To avoid misdiagnosis, doctors are advised to carry out other tests and examinations to rule out conditions with similar symptoms, such as thrush and vaginismus. For example, the presence of tight pelvic muscles upon internal examination of the vagina may indicate that the diagnosis is more likely to be vaginismus. Thrush can present similarly but may be identified by vaginal swabs. It is important to avoid a misdiagnosis of thrush as repeated anti-thrush treatments can exacerbate vestibulodynia.4
Causes and risk factors
Currently, there is no known, identifiable cause of vestibulodynia, with prominent theories consisting of hypersensitive nerve endings or overgrown nerve fibres in the vestibule.16
However, external risk factors may trigger or exacerbate the condition. Physical vaginal injury caused by childbirth, surgery, or sexual abuse can contribute to pain in the vulvar vestibule. Vulvar dermatitis (inflammation) caused by irritants like detergents, soaps, douches, and panty liners may also play a role. The onset of vestibulodynia may occur following chronic yeast infections such as thrush and/or in response to long-term anti-thrush treatment.7
Novel theories on vestibulodynia and vulvodynia adopt a neurobiological perspective, postulating hormonal imbalances and a genetic predisposition as the cause. For example, low levels of oestrogen may contribute to the onset of vestibulodynia. This theory is based on reports of vulvar pain following the use of combined hormonal contraceptives, which can alter the function of the vestibular mucosa, causing hypersensitivity in response to mechanical stress. 8 Studies have also reported that some people AFAB going through menopause also experience vulvar pain, which supports the theory that low oestrogen levels may contribute to vulvodynia and vestibulodynia.9
It has also been suggested that some people with AFAB have a genetic predisposition to provoked vestibulodynia. This is most likely related to genetic polymorphism that increases the likelihood of vulvar infections or exaggerated inflammatory responses. 10 Some studies undermine this theory of genetic polymorphism, and thus, it is unclear whether genetic risk factors play a role in vestibulodynia.11 Hopefully, future studies will be able to identify the risk alleles and candidate genes responsible.
Some patients suffering from vestibulodynia also suffer from psychological disorders such as anxiety, depression, and algophobia (fear of pain).12 This link suggests that pain perception can be heightened by psychological factors, which is not to negate the devastating experience that patients suffering from vestibulodynia experience but indicates that psychotherapy may be a useful treatment option.13
Treatment options
Unfortunately, due to the lack of understanding regarding the cause of vestibulodynia, there is no definitive treatment option. Current treatment methods target the symptoms and potential comorbidities occurring alongside vestibulodynia. Patients are advised to opt for lifestyle changes and combination therapy that is personalised to the individual, depending on the symptoms and their severity.
Preventative action
Preventative action and self-coping strategies are usually the first steps in the treatment of vestibulodynia to avoid further exacerbating the condition. It is recommended to discontinue the use of irritant products such as soaps, detergents, feminine hygiene products, and bubble baths. If a soap or detergent must be used, consult with your doctor and use dermatologically approved products. One suggestion is to avoid douching and, instead, gently rinse the vulva with lukewarm water to keep the area clean. Wear loose-fitting underwear and pants instead of tight-fitting ones to avoid physical irritation. Limit irritating physical activities, in particular, cycling, which puts pressure on the vulva and any intense activities, such as running, which may generate friction in the vulvar area. For individuals who experience provoked vestibulodynia after sexual intercourse, try to avoid sexual acts involving the vulvar region completely until the vestibule is restored to its healthy state. It may be useful to use water-based lubricants, try more comfortable sexual positions and avoid using contraceptive creams and spermicides.
Non-pharmacological treatment
The next step following preventative care is to consult a healthcare professional who can provide education on all therapeutic options. Non-pharmacological therapies, including pelvic floor muscle exercise and the use of biofeedback machines, may prove useful in alleviating the symptoms of vestibulodynia. For patients with the condition who experience pelvic floor muscle weakness or spasms, pelvic floor physical therapy can help relax the vaginal muscles and relieve hypersensitivity felt in the affected area. Biofeedback machines can be used to monitor the strength of the pelvic floor muscles.6,14
Pharmacological treatment
Oral or topical medications are available from your doctor and over the counter to help alleviate the symptoms of vestibulodynia. Topical creams can directly be applied to the vulva and vestibule to ease the pain. Topical hormone creams containing oestrogen can help adjust hormonal imbalances and improve the health of vulvar tissue. Local anaesthetics such as lidocaine can be applied to the sensitive area to numb the tissue temporarily. 5% lidocaine can be bought over the counter; however, in the case of intense chronic pain and if more pain relief is needed, your doctor can prescribe oral analgesics. These include tricyclic antidepressants (TCAs) such as amitriptyline and nortriptyline, serotonin-noradrenaline reuptake inhibitors (SNRIs), anticonvulsants such as gabapentin and pregabalin, and opioids such as oxycodone and hydrocodone. 6
Surgery
In rare and extreme cases, the only option left for the treatment of vestibulodynia is surgical intervention. Doctors may recommend one of two surgeries: a modified vestibulectomy or a vestibulectomy with vaginal advancement. The former includes removal of the vestibule, whereas the latter involves an additional vaginal advancement. 6
Support
Chronic pain conditions can have detrimental effects on both physical and mental well-being. Alongside treatment plans, there are support resources available to help patients cope with pain management. Cognitive behavioural therapy (CBT) focuses on improving your state of mind to cope with the disorder. If vestibulodynia significantly affects your sexual relations with your partner, psychosexual counselling can help manage your fear and anxiety regarding sex and restore a healthy physical relationship. To help cope with the long-term effects of vestibulodynia, support groups are available to help patients find a community with other patients who share the same experiences. The Vulval Pain Society and Pelvic Pain Support Network are two of the largest support groups you can contact14
Prognosis and outlook
Despite a lack of understanding of the cause of vestibulodynia, with proper treatment and support, most patients initially experience a natural remission from this condition. Evidence suggests that physical and psychological therapies generate positive outlooks.15 Unfortunately, it is still currently observed that most people with AFAB suffering from vulvodynia (approximately 50% of remitters) undergo relapse within 6-30 months.17 Hopefully, future research on the underlying cause of vulvodynia and vestibulodynia may provide perspective into more effective treatment.
Summary
Vestibulodynia is a common disorder that causes pain and discomfort in the vestibular region of the vulva. Pain occurs when the area is lightly touched, along with other primary symptoms, including redness and inflammation. Diagnosis typically includes physical examination and tests. The definitive cause of vestibulodynia is still unknown. However, risk factors such as physical injury and irritation, biological differences and infections can exacerbate the condition. Early diagnosis of this condition is extremely important as, with the correct intervention, it is easily treated and preventable. Consult with a healthcare professional to get started on a treatment plan, which may involve preventive care, non-pharmacological therapies, medication and surgery. For extra support, patients can seek help from therapists and counsellors, as well as joining support groups. Treatment plans are normally successful. However, there is still the problem of relapse. Due to the chronic nature of vestibulodynia and its likelihood of relapse, it is unlikely that a ‘cure’ for vestibulodynia will ever be found. However, there is promising ongoing research which will educate healthcare professionals and patients on more suitable, effective therapies to deal with pain management.
References
- Vulvodynia and vestibulodynia. British Association of Dermatologists; 2021. Available from: https://www.bad.org.uk/pils/vulvodynia-and-vestibulodynia/ (Accessed: 27 October 2023).
- Vulvar Vestibulitis.The Centres for Vulvovaginal Disorders. Available from: https://vulvodynia.com/conditions/vulvar-vestibulitis (Accessed: 27 October 2023).
- Reed BD, Harlow SD, Sen A, Legocki LJ, Edwards RM, Arato N, et al. Prevalence and demographic characteristics of vulvodynia in a population-based sample. Am J Obstet Gynecol. 2012 Feb;206(2):170.e1-9.
- Vestibulodynia. NHS choices. Available from: https://www.hey.nhs.uk/patient-leaflet/vestibulodynia (Accessed: 27 October 2023).
- Vieira-Baptista P, Lima-Silva J, Pérez-López FR, Preti M, Bornstein J. Vulvodynia: A disease commonly hidden in plain sight. Case Rep Womens Health. 2018 Oct;20:e00079.
- Nguyen JD, Duong H. Anatomy, Abdomen and Pelvis: Female External Genitalia. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Oct 27]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK547703/
- Oakley A, Ngan V. Vestibulodynia. 2017. Available from: https://dermnetnz.org/topics/vestibulodynia
- Bazin S, Bouchard C, Brisson J, Morin C, Meisels A, Fortier M. Vulvar vestibulitis syndrome: an exploratory case-control study. Obstet Gynecol. 1994 Jan;83(1):47–50.
- Torres-Cueco R, Nohales-Alfonso F. Vulvodynia-It Is Time to Accept a New Understanding from a Neurobiological Perspective. Int J Environ Res Public Health. 2021 Jun 21;18(12):6639.
- Goldstein AT, Belkin ZR, Krapf JM, Song W, Khera M, Jutrzonka SL, et al. Polymorphisms of the androgen receptor gene and hormonal contraceptive induced provoked vestibulodynia. J Sex Med. 2014 Nov;11(11):2764–71.
- Heddini U, Bohm-Starke N, Grönbladh A, Nyberg F, Nilsson KW, Johannesson U. GCH1-polymorphism and pain sensitivity among women with provoked vestibulodynia. Mol Pain. 2012 Sep 12;8:68.
- Sutton K, Pukall C, Wild C, Johnsrude I, Chamberlain S. Cognitive, psychophysical, and neural correlates of vulvar pain in primary and secondary provoked vestibulodynia: a pilot study. J Sex Med. 2015 May;12(5):1283–97.
- Mascherpa F, Bogliatto F, Lynch PJ, Micheletti L, Benedetto C. Vulvodynia as a possible somatization disorder. More than just an opinion. J Reprod Med. 2007 Feb;52(2):107–10.
- Vulvodynia. NHS choices. Available from: https://www.nhs.uk/conditions/vulvodynia/ (Accessed: 27 October 2023).
- Henzell H, Berzins K, Langford JP. Provoked vestibulodynia: current perspectives. Int J Womens Health. 2017;9:631–42.
- Vestibulodynia. Baylor College of Medicine. Available from: https://www.bcm.edu/healthcare/specialties/obstetrics-and-gynecology/ob-gyn-conditions/vestibulodynia (Accessed: 27 October 2023).
- Reed BD, Harlow SD, Plegue MA, Sen A. Remission, Relapse, and Persistence of Vulvodynia: A Longitudinal Population-Based Study. J Womens Health (Larchmt). 2016 Mar;25(3):276–83.




