


Introduction
The process of giving birth is challenging and exhausting. Many hormonal, physical, emotional, and psychological changes occur during pregnancy. The birthing parent’s social and familial environment undergoes a profound transformation. They may feel a range of feelings following childbirth, from happiness and pleasure to sorrow and fits of sobbing.
Postpartum depression (PPD) affects around one in seven people assigned female at birth (AFAB). While a birthing parent experiencing typical ‘baby blues’ tends to recover quickly, PPD severely affects their ability to return to normality.
PPD has an effect on the birthing parent’s bond with their child. PPD is also associated with impaired maternal brain reactivity and behaviour. Privacy conflicts and a desire to keep information from close family members prevent up to half of PPD diagnoses among new birthing parents.1
Postpartum period
The three distinct but continuous phases of the postpartum period are termed the "fourth stage of labour", displayed in the table below.
| Phases | Change |
| Initial or acute period (6-12 hours postpartum) | There is a possibility for acute conditions such as eclampsia, uterine inversion, amniotic fluid embolism (AFE), and postpartum haemorrhage (PPH) during this period of rapid transformation |
| Subacute postpartum period (lasts 2-6 weeks) | The body goes through significant changes involving metabolism, genitourinary recovery, emotional state, and haemodynamics. However, compared to the acute postpartum phase, the changes occur more slowly, and the patient can recognise concerns themselves |
| Prolonged postpartum period (lasting for six months) | Pathology is rare at this phase, and changes occur gradually.At this time, connective tissue and muscle tone will return to their pre-pregnant levels. During this phase, changes are slight, but caretakers must remember that a body does not entirely return to its pre-pregnant physiology until approximately six months after birth2 |
PPD has many different and complex causes, including social, psychological, emotional, and physiological elements. In the next part of the article, let's take a more in-depth look at the several factors that can contribute to PPD.
Hormonal fluctuations
Hormonal changes after childbirth
- Oestrogens (estradiol, estriol, and estrone) and progesterone are produced primarily by the placenta during pregnancy, which causes a steady rise in these hormone levels. Oestrogen and progesterone levels fall dramatically after birth and revert to pregravid (pre-pregnancy) levels by the fifth postpartum day
- Human chorionic gonadotrophin (HCG), cortisol and beta-endorphin levels all increase throughout pregnancy, peaking close to term and then falling before delivery
- Pregnancy-related high oestrogen levels increase the thyroid hormone-binding globulin produced, which causes a decrease in free T3 (triiodothyronine) and T4 (thyroxine) and an increase in bound T3 and T4 levels. Thyroid-stimulating hormone (TSH) rises, making up for the low levels of free thyroid hormones; free T3 and T4 stay within the normal range
- Total and free T3 and T4 levels drop after delivery due to a decline in thyroid-binding globulin, but the former stays stable. The blood levels of prolactin increase during pregnancy, reaching their maximum after childbirth, and, in an those who are not lactating, return to pregravid levels three weeks later
- Breastfeeding keeps prolactin levels high by stimulating pituitary lactotrophic cells to produce oxytocin. However, prolactin levels gradually revert to pregravid levels even in nursing birthing parents
As seen in the graphic below, there are notable hormonal variations that can impact mood control and exacerbate PPD.
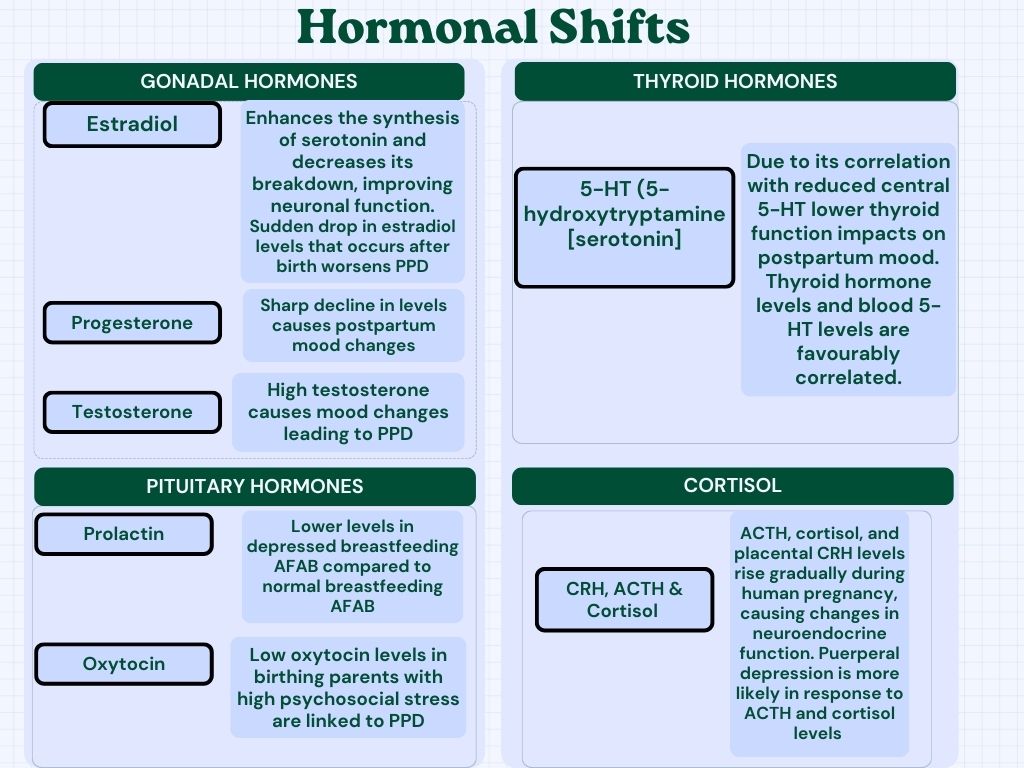
Testosterone, 5 hydroxytryptamines (serotonin), placental corticotropin-releasing hormone (CRH), adrenocorticotropic hormone (ACTH) and puerperal depression
Created by: Deepika Rana (Canva)3,4
Risk factors
Emotional factors
Physiological changes and family commitments may account for the elevated frequency of fatigue among birthing parents. Birthing parents' reports of being exhausted after giving birth are associated with having a newborn that has erratic sleeping patterns, cries for no apparent reason, and wakes up a lot to feed.
Fatigue and tiredness result from the birthing parents' lack of sleep during this crucial transition period. Furthermore, there was a positive correlation found between low sleep quality and characteristics like PPD, work, the baby's sex, home birth, pre-natal mental illness, and medical issues after delivery. Pregnant and postpartum individuals showed low levels of resilience.5
Stressful life events
- For several expectant birthing parents, pregnancy might be a difficult period. Acute, stressful situations like losing a job or losing a loved one can also occur for some during pregnancy
- Birthing parents reporting stresses linked to trauma had the highest prevalence of PPD, followed by stressors related to relationships, finances, and emotions. After adjusting for confounders, the birthing parent's younger age (less than 20 years old), low income (less than $10,000), and marital status (married) proved to be independently related to a higher chance of PPD10
Psychological factors
Pregnancy-related mental health conditions, including depression, are a strong predictor of PPD. The serotonin transport system and the serotonin transporter polymorphism region are related to serious depression in women who suffer from severe pre-menstrual syndrome (PMS).
Tryptophan deficiency and the onset of significant depression after childbirth can result from high serotonin polymorphism. A history of sexual abuse in the past, life events, low self-esteem (with an impact on parenting stress), and a negative attitude towards the pregnancy were all predisposing risk factors for PPD, in addition to past history of depression.6
Social and environmental factors
The visual below provides the finest representation of social support.

Created by: Deepika Rana (Created with BioRender.com)
- The most significant environmental component associated with the emergence of anxiety and depression is a reduction in social support. Decision-making authority at home and enhanced partner support are critical solution strategies to improve reproductive health
- Pregnancy-related domestic abuse, including sexual assault by a spouse, is a contributing factor to the prevalence of PPD
- Social factors attributed to a 1.7-fold increase in the occurrence of PPD, including smoking during pregnancy, in addition to the person’s relationships with their family and community
- Pregnancy-related physiological changes, however, might cause some to experience stress, which can result in the emergence of depressive symptoms and the start of smoking
- Work status is another social component. Professional occupations, in particular, have been linked to a lower risk of PPD. On the other hand, low income and low education correlate with a higher risk of PPD6
Cultural and societal influences
- Certain societies have an idealised view of parenting, putting pressure on new birthing parents to live up to these standards. There are stigmatising attitudes and ideas about PPD in the parental community
- PPD often goes unnoticed or undiagnosed because the individual typically reports feeling guilty about getting treatment and worries about being viewed as "bad” birthing parents if they admit they are struggling with depression. Good anti-stigma tactics include promoting equality in relationships between the general public and those who suffer from mental illnesses
- Social media platforms today have a significant impact on people's body image problems. Social media can affect people’s perceptions of their bodies during and after pregnancy in both positive and negative ways11,12
Physical health and recovery
The physical discomfort, effects of medical issues during pregnancy or delivery, and challenges in resuming routine physical activities can cause PPD, as illustrated in the table below.
| Factors | Explanation |
| Number of deliveries | PPD is more common in multiparous birthing parents than in nulliparous, according to research by Mayberry et al. Having two or more children due to a higher psychological burden is more likely to be connected with the onset of depression, according to research conducted in 2013 by Matsin on 86 participants within six weeks of delivery |
| Risky pregnancy | These risks include circumstances that necessitate an emergency caesarean section or hospitalisation during pregnancy. Postpartum complications such as meconium passage, umbilical cord prolapse, and obstetric haemorrhages assist in the incidence of PPD. PPD is more likely to affect birthing parents who give birth to a newborn weighing less than 1500 g, ranging from 4 to 18 times higher than other birthing parents |
| Birth expectations | According to reports, those who desire a normal birth during the perinatal period but end up having a caesarean section are at a higher risk of developing PPD |
| Low haemoglobin concentration on the 7th day after delivery (<120 g/L) | Associated with symptoms of PPD 28 days following birth. Furthermore, a significant association exists between depression and homocysteinemia in the first and sixth weeks following delivery |
| Resuming physical exercises is tough | The failure to return to routine daily activities harms a postpartum person's emotional health. Frequent exercise reduces the chance of depression during pregnancy and is a secure preventative measure6,9 |
Biological and genetic factors
A visual with a simplified explanation of these factors
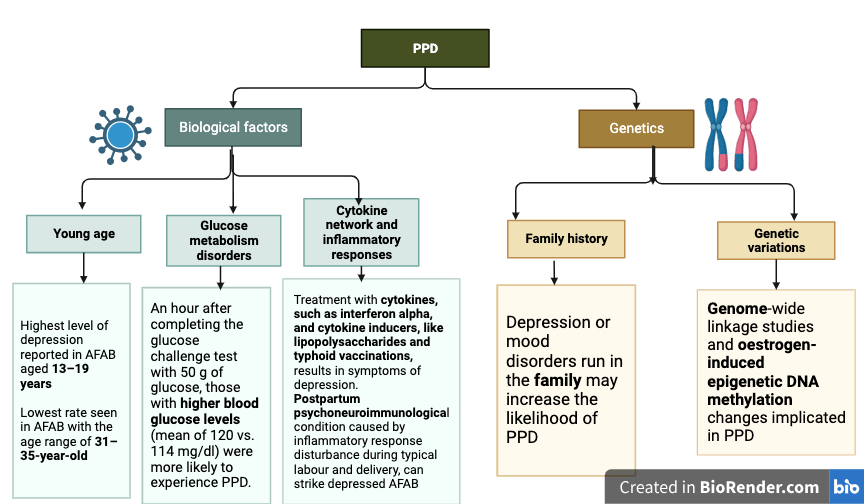
Glucose metabolism disorders, glucose challenge test, cytokine, typhoid vaccinations, inflammatory response and oestrogen-induced epigenetic DNA methylation
Created by: Deepika Rana6,8 (Created with BioRender.com)
FAQ's
How many people get PPD?
Between 6.5% and 20% of birthing parents experience PPD. Adolescent birthing parents, parents who give birth to premature babies, and city dwellers are the populations most likely to experience it. According to one study, white birthing parents reported symptoms starting later, but African-American and Hispanic birthing parents showed symptoms within two weeks of delivery.1
What is the duration of PPD?
PPD has varying natural duration. The majority of PPD cases go away with treatment in a matter of months, however around 13% to 24% of birthing parents with the diagnosis continue to experience depression two years after giving a child. About 40% of people with PPD will relapse, either unrelated to or during a second pregnancy. If PPD is left untreated, depressed episodes may return often, causing complications for the birthing parent, child, and family.8
Can PPD affect fathers?
The first two months after giving birth are estimated to have a 4–25% prevalence of paternal postpartum depression, depending on estimates. In addition to having a high degree of comorbidity with maternal PPD, paternal PPD is responsible for other postpartum psychiatric conditions.7
Summary
Acknowledging these complex causes of PPD is essential for prompt detection, intervention, and assistance. By addressing these issues, getting expert advice, and establishing robust support networks, PPD's effects are notably decreased. It's critical to keep in mind that PPD is a treatable condition and that impacted birthing parents and their families can heal with the correct assistance.
References
- Mughal S, Azhar Y, Siddiqui W. Postpartum depression. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Nov 6]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK519070/
- Romano M, Cacciatore A, Giordano R, La Rosa B. Postpartum period: three distinct but continuous phases. J Prenat Med [Internet]. 2010 [cited 2023 Nov 6];4(2):22–5. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3279173/
- Hendrick V, Altshuler LL, Suri R. Hormonal changes in the postpartum and implications for postpartum depression. Psychosomatics [Internet]. 1998 Mar 1 [cited 2023 Nov 7];39(2):93–101. Available from: https://www.sciencedirect.com/science/article/pii/S0033318298713556
- Trifu S, Vladuti A, Popescu A. The neuroendocrinological aspects of pregnancy and postpartum depression. Acta Endocrinol (Buchar) [Internet]. 2019 [cited 2023 Nov 7];15(3):410–5. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6992410/
- Baattaiah BA, Alharbi MD, Babteen NM, Al-Maqbool HM, Babgi FA, Albatati AA. The relationship between fatigue, sleep quality, resilience, and the risk of postpartum depression: an emphasis on maternal mental health. BMC Psychology [Internet]. 2023 Jan 13 [cited 2023 Nov 7];11(1):10. Available from: https://doi.org/10.1186/s40359-023-01043-3
- Ghaedrahmati M, Kazemi A, Kheirabadi G, Ebrahimi A, Bahrami M. Postpartum depression risk factors: A narrative review. J Educ Health Promot [Internet]. 2017 Aug 9 [cited 2023 Nov 7];6:60. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5561681/
- Kim P, Swain JE. Sad dads. Psychiatry (Edgmont) [Internet]. 2007 Feb [cited 2023 Nov 7];4(2):35–47. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2922346/
- Stewart DE, Vigod SN. Postpartum depression: pathophysiology, treatment, and emerging therapeutics. Annu Rev Med [Internet]. 2019 Jan 27 [cited 2023 Nov 8];70(1):183–96. Available from: https://www.annualreviews.org/doi/10.1146/annurev-med-041217-011106
- Kołomańska-Bogucka D, Mazur-Bialy AI. Physical activity and the occurrence of postnatal depression—a systematic review. Medicina (Kaunas) [Internet]. 2019 Sep 2 [cited 2023 Nov 8];55(9):560. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6780177/
- Qobadi M, Collier C, Zhang L. The effect of stressful life events on postpartum depression: findings from the 2009–2011 Mississippi pregnancy risk assessment monitoring system. Matern Child Health J [Internet]. 2016 [cited 2023 Nov 8];20(Suppl 1):164–72. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5290058/
- Thorsteinsson EB, Loi NM, Farr K. Changes in stigma and help-seeking in relation to postpartum depression: non-clinical parenting intervention sample - PMC [Internet]. PubMed Central (PMC). 2018 [cited 2023 Nov 8]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6230434/
- Trehan A, Sehgal SS. Effect of social media on body image of pregnant and postpartum women in India. Health Care for Women International [Internet]. 2023 Oct 23 [cited 2023 Nov 8];1–20. Available from: https://www.tandfonline.com/doi/full/10.1080/07399332.2023.2267007




