

Bariatric surgery, also known as weight loss surgery, has proven to be an efficient method for shedding excess weight and achieving remission in type 2 diabetes. It induces weight-loss, hormonal and gut microbiota changes which improves insulin sensitivity and glycemic control.
Obesity and diabetes have an inseparable relationship. The benefits of bariatric surgery can be weight loss dependent and independent. Despite the affirmative aspects of this surgical approach, careful consideration of eligibility criteria and potential risks is imperative before reaching a definitive judgment on whether its merits outweigh the drawbacks.
Introduction
Type 2 diabetes (T2DM) is a chronic (long-term) disease where the mechanism of blood sugar (glucose) level control is impaired, and the body cannot lower the blood sugar level. One of the blood sugar level-controlling hormones in our body is insulin. In patients with T2DM, their pancreas cannot produce enough insulin, or their organs cannot respond well to insulin.
Obesity is a significant risk factor for diabetes. Statistics have shown that 85% of patients with T2DM are overweight.1 These conditions, often referred to as twin epidemics, have become prevalent on a global scale, affecting millions of individuals of all ages. The significant increase in diabetes. and obesity prevalence has prompted a growing urgency to explore innovative approaches to manage and, ideally, alleviate their impact on public health.
One such approach that has garnered considerable attention is the relationship between bariatric surgery and diabetes. The intriguing connection between these two seemingly distinct domains has opened up new avenues for understanding and addressing these health concerns. As researchers and medical practitioners delve deeper into this relationship, the potential of bariatric surgery to not only address obesity but also influence diabetes management has become increasingly significant. A randomized controlled trial at the University of Pittsburgh compared patient T2DM emission with and without bariatric surgical interventions for 5 years. They showed that patients who underwent bariatric surgical treatments had more significantly reduced weight and reduced need for medication for T2DM.2
In this exploration, we aim to uncover the complex interplay between bariatric surgery and diabetes, shedding light on the potential benefits and considerations associated with this evolving field of healthcare.
Understanding bariatric surgery
There are many types of bariatric surgeries and the doctor can choose to accord with the patient's situation. Common types of bariatric surgery include Roux-en-Y gastric bypass (RYGB), Vascular Sleeve Gastrectomy (VSG), and Gastric banding.
Gastric Bypass (Roux-en-Y)
Figure 1. Roux-en-Y Gastric bypass3
The gastric bypass procedure, often referred to as Roux-en-Y gastric bypass, is one of the most well-established and commonly performed bariatric surgeries. There are four main steps of this surgery. This surgical intervention involves the creation of a small stomach pouch, effectively limiting the amount of food an individual can consume. The small intestine is then rearranged to connect directly to this pouch, bypassing a significant portion of the stomach and the upper intestine.4
The remarkable aspect of gastric bypass surgery is its multifaceted impact. It not only restricts food intake because of the reduced stomach size but also leads to altered nutrient absorption in the intestine. This method is one of the bariatric surgeries that is beneficial to diabetes as it shows normalization of insulin resistance in severely obese patients.5
Vascular Sleeve Gastrectomy
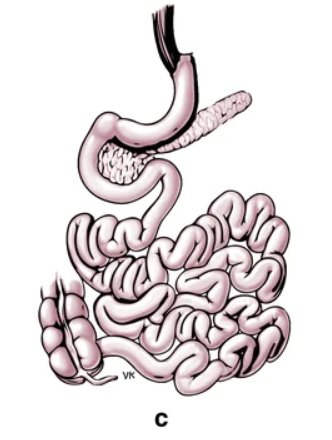
Figure 2. Vascular Sleeve Gastrectomy3
Vascular Sleeve gastrectomy (VSG), another widely performed bariatric procedure, involves the removal of a significant portion of the stomach, leaving behind a slender, tube-shaped stomach resembling a "sleeve." This reduction in stomach size leads to a reduced capacity for food consumption6, as well as alterations in hunger-related hormones like GLP-1.7
The sleeve gastrectomy's primary mechanism is the restriction of food intake, which naturally leads to weight loss. The procedure appears to positively influence metabolic factors, including blood glucose regulation and insulin sensitivity, which applies to individuals with diabetes.5
Adjustable Gastric Banding (Lap-Band)

Figure 3. Laparoscopic Adjustable Gastric Banding3
Adjustable gastric banding, commonly recognised by the brand name Lap-Band, employs a different approach compared to the previously mentioned procedures. In this minimally invasive surgery, an adjustable band is placed around the upper part of the stomach, creating a small pouch. The band is adjustable by adding or removing the liquid from the balloon around the band.8
The key feature of this procedure is adjustability. By modifying the tightness of the band, healthcare professionals can control the rate of food passage from the pouch to the remainder of the stomach. This adjustable aspect offers a level of flexibility in terms of weight loss and metabolic outcomes.9
Why is bariatric surgery good for diabetics?
The two main types of bariatric surgeries that are beneficial to T2DM are RYGB and VSG. The exact mechanism behind their mode of action requires debate but there are many improvements in patients after surgery. Weight loss, hormonal change and remission of insulin sensitivity result in the merits shown in the patients.
Weight loss
The primary purpose of bariatric surgery is to achieve weight loss. There are weight-loss-dependent mechanisms for T2DM remission. Weight loss improves glucose control in patients after surgery by increasing insulin sensitivity, which means the organs can better respond to insulin secreted by the pancreas/10
Hormonal change
VSG and RYGB both reduce stomach size and lead to rapid stomach clearance and speed up intestinal transit, which can cause hormonal changes. Hormones like Glucagon-like peptide 1 (GLP-1), Ghrelin and Leptin alter their secretion patterns in response to the surgical procedure. The surgery produced a rise in GLP-1, GLP-1 promotes insulin secretion and inhibits glucagon secretion.7 Ghrelin is a neuropeptide that can suppress insulin secretion, which decreases its level post-surgery. Leptin is a hormone secreted by adipose tissue which acts on the brain to control appetite.7 Leptin level decreases after VSG and RYGB but it is thought to be weight loss dependent. However, some patients after bariatric surgery show increased satiety, which leads to a hypothesis that leptin sensitivity increases after surgery.11
Others
There are other weight-loss independent reasons behind the benefits of bariatric surgery. The surgery induces a shift of gut microbiota from “good” to “bad” which changes bile acid metabolism, food intake preference and even neural function over time.10 Scientists also recorded cortisol level change after VSG and it may contribute to the mechanism as patients with obesity often have dysregulated cortisol levels/12
Patient selection and criteria
Patient selection and criteria play a pivotal role in the success and safety of bariatric surgery. It's crucial to carefully evaluate individuals to ensure they are suitable candidates for these transformative procedures. Not everyone is eligible for bariatric surgery, and eligibility criteria typically include factors such as body mass index (BMI), previous weight loss attempts, and overall health.
Currently, a classic criteria for bariatric surgery is BMI≥40 or BMI≥35 with at least one obesity-related condition. Only patients with BMI≥35 and uncontrolled T2DM can be considered for bariatric surgery.6
For individuals with diabetes, particularly type 2 diabetes, bariatric surgery presents a potential solution. However, specific guidelines apply to diabetes patients, taking into account factors like glycemic control, medication management, and the presence of diabetes-related complications. These guidelines help determine the suitability of surgery as an intervention and guide the medical team in optimizing the procedure for diabetes management.
What are the disadvantages of weight loss surgery for diabetes?
While weight loss surgery has shown promise in addressing diabetes, it is essential to acknowledge the potential risks associated with these procedures.
There are surgical risks like an anastomotic leak, stricture, and gastroesophageal reflux, leading to symptoms like vomiting, significantly increased heart rate and nausea. However, these incidents of these risks are within 5% of patients.6
Weight loss surgery often leads to substantial changes in the gastrointestinal tract, impacting nutrient absorption. Patients may face challenges in maintaining proper nutrition, including vitamin and mineral deficiencies. This can be controlled or prevented by routine testing and regular dietary supplement intake.6
Although studies are showing promising results for T2DM remission after bariatric surgery, more experiments and controlled clinical studies are required for better treatment strategies. The cost-effectiveness data are still missing and long-term post-surgery control remains unclear.3
Summary
Bariatric surgery is a surgical process focusing on weight loss but recent research has found its benefits for patients with T2DM. VSG and RYGB are two main kinds of bariatric surgery that are suitable for patients with T2DM. It improves insulin sensitivity, blood sugar control and reduces the risk of other complications. However, not all patients meet the criteria for bariatric surgery and surgical risk should be evaluated before any decisions.
In summary, bariatric surgery stands as a remarkable and evolving approach in the realm of diabetes management. It offers hope, renewed health, and improved quality of life for many individuals, but it also underscores the importance of personalized care and the careful weighing of advantages and disadvantages. As we continue to navigate the dynamic landscape of healthcare, the relationship between bariatric surgery and diabetes remains a compelling and evolving field, promising new horizons for those living with this challenging metabolic condition.
References
- EmmaW. Weight loss and diabetes [Internet]. Diabetes UK; [cited 2023 Oct 27]. Available from: https://www.diabetes.org.uk/guide-to-diabetes/enjoy-food/eating-with-diabetes/whats-your-healthy-weight/lose-weight
- Courcoulas AP, Gallagher JW, Neiberg RH, Eagleton EB, DeLany JP, Lang W, et al. Bariatric surgery vs Lifestyle Intervention for Diabetes Treatment: 5-year outcomes from a randomized trial. The Journal of Clinical Endocrinology & Metabolism. 2020;105(3):866–76. doi:10.1210/clinem/dgaa006
- Koliaki C, Liatis S, le Roux CW, Kokkinos A. The role of bariatric surgery to treat diabetes: Current challenges and Perspectives. BMC Endocrine Disorders. 2017;17(1). doi:10.1186/s12902-017-0202-6
- Mitchell BG, Gupta N. Roux-en-Y Gastric Bypass. [Updated 2023 Jul 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553157/
- Benaiges D, Flores Le-Roux JA, Pedro-Botet J, Chillarón JJ, Renard M, Parri A, et al. Sleeve gastrectomy and roux-en-Y gastric bypass are equally effective in correcting insulin resistance. International Journal of Surgery. 2013;11(4):309–13. doi:10.1016/j.ijsu.2013.02.007
- Seeras K, Sankararaman S, Lopez PP. Sleeve Gastrectomy. [Updated 2023 Jan 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK519035/
- Benaiges D. Laparoscopic sleeve gastrectomy: More than a restrictive bariatric surgery procedure? World Journal of Gastroenterology. 2015;21(41):11804. doi:10.3748/wjg.v21.i41.11804
- 8.Laparoscopic adjustable gastric banding [Internet]. 2021 [cited 2023 Oct 27]. Available from: https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/laparoscopic-adjustable-gastric-banding
- Seeras K, Acho RJ, Prakash S. Laparoscopic Gastric Band Placement. [Updated 2023 Jan 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526062/
- Sandoval DA, Patti ME. Glucose metabolism after bariatric surgery: Implications for T2DM remission and hypoglycaemia. Nature Reviews Endocrinology. 2022;19(3):164–76. doi:10.1038/s41574-022-00757-5
- Arble DM, Sandoval DA, Seeley RJ. Mechanisms underlying weight loss and metabolic improvements in rodent models of bariatric surgery. Diabetologia. 2014;58(2):211–20. doi:10.1007/s00125-014-3433-3
- Akalestou E, Lopez-Noriega L, Christakis I, Hu M, Miras AD, Leclerc I, et al. Vertical sleeve gastrectomy normalizes circulating glucocorticoid levels and lowers glucocorticoid action tissue-selectively in mice. Frontiers in Endocrinology. 2022;13. doi:10.3389/fendo.2022.1020576




