What are kidneys and their function?
Kidneys are the two bean-shaped organs, approximately the size of a fist, located just below the rib cage on each side of the spine. They are responsible for filtering blood through a network of filtering units called the nephrons, where each nephron filters a small amount of blood. The nephron is composed of two structures called glomerulus and renal tubule. The filtration rate depends on individuals and is less in children compared to adults. The filtration process involves the elimination of fluid and waste products from the blood, and the retention of important minerals and nutrients like sodium, potassium, salts, proteins etc., sending the filtered blood back to the circulatory system. The unwanted waste products are eliminated from the blood circulation in the form of urine, through the urinary tract (urethra).
Short-term or permanent damage to the kidneys may result in the disruption of this process, ranging from curable long-term conditions to life-threatening consequences.
Types of Kidney Disease
Based on the method of development, kidney (renal) disorders can be of two types:
- Acute Kidney Injury (AKI): develops suddenly, lasts a short time, and may have long-term consequences, although these consequences can potentially be cured depending on the underlying cause.
- Chronic Kidney Disease (CKD): is not curable and develops further over time, eventually leading to kidney (renal) failure, known as End-Stage Renal Disease (ESRD). ESRD needs to be treated with a kidney transplant or an artificial blood filtration technique called dialysis.
The following figure describes the progression of kidney disease from birth to adolescence in children and the complications associated with it.
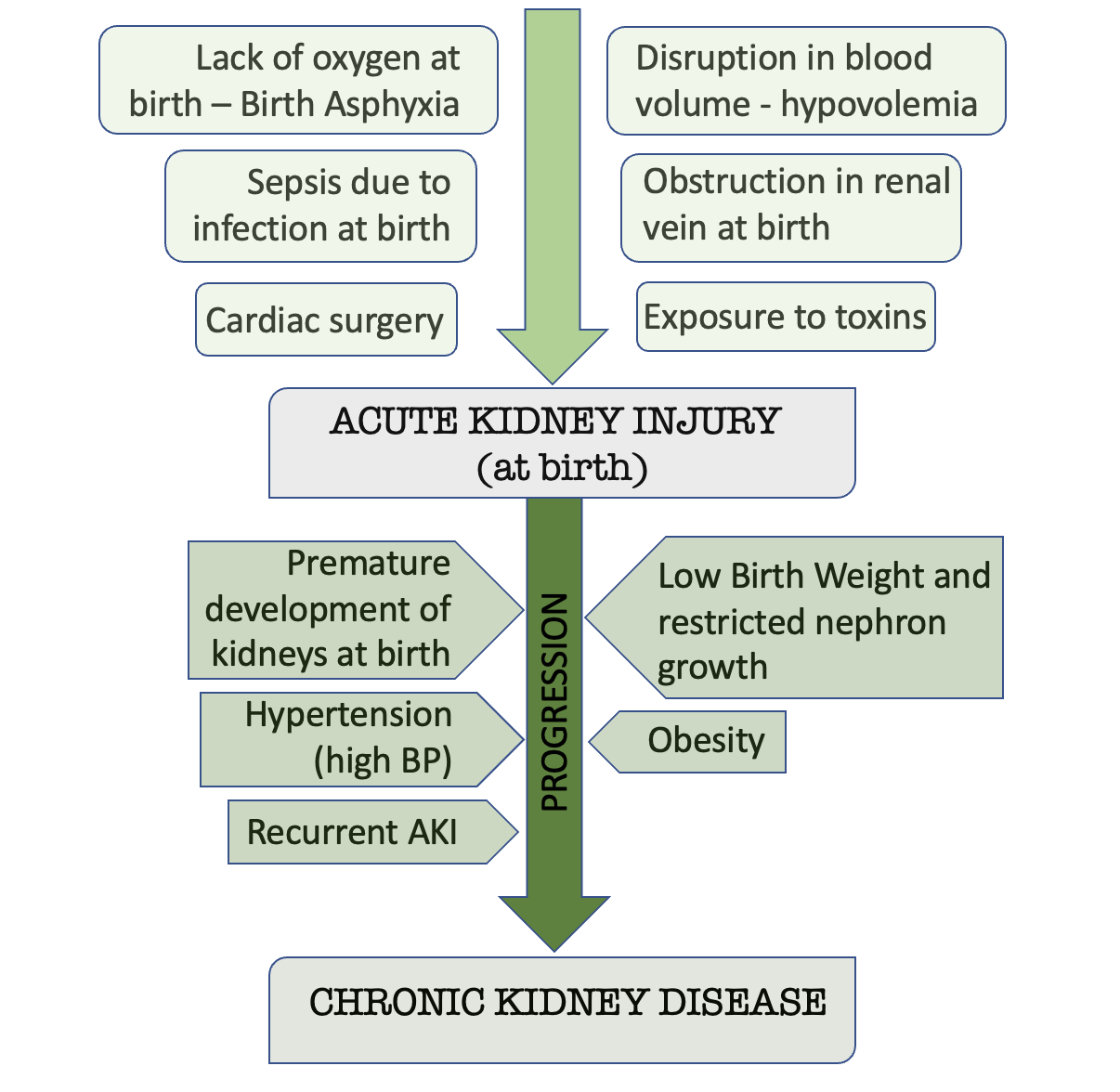
Figure 1. Progression of kidney disease from birth to adolescence and associated complications.1
Underlying causes of these disorders in children are1:
- Birth defects
- Hereditary diseases
- Infection
- Nephrotic syndrome
- Systemic disease
- Trauma
- Urine blockage or reflux
Birth defects
This refers to the complications that can arise during the development of the baby in the mother’s womb, or during childbirth. They may range from abnormalities of size, structure, or position of kidneys to functional damage. These are known as:
- Renal agenesis – children born with only one kidney
- Renal dysplasia – children born with two kidneys, yet only one functions
- Ectopic kidney – children born with a kidney not in its normal position
Children born with these defects are at increased risk of developing kidney disease in future. Doctors can diagnose it before or just after birth and can treat it with surgery.
Hereditary defects
Polycystic Kidney Disease (PKD)
PKD is characterised by the presence of round fluid-filled cysts (abnormal sacs which grow and increase the size of the kidneys over time), which eventually damage the kidney tissues and render them non-functional. Usually, there are no significant symptoms until the cysts develop to disrupt kidney function later on in life (30-60 years of age). Some signs include:
- stomach aches
- high blood pressure (hypertension)
- blood in the urine (haematuria), detected only through urine tests and not the naked eye
- potentially serious upper urinary tract infection (UTIs)
- kidney stones
These lead to the deterioration of kidney function, followed by complete kidney failure.
Multicystic Kidney Disorder (MKD)
MKD is characterised by the development of large cysts in the kidney (like PKD) that disrupts the proper kidney function and lead to complete kidney failure. The difference between PKD and MKD is that PKD affects both kidneys, whereas MKD affects just one kidney. It is a rare inherited disorder (200 cases worldwide) that develops in children younger than 1 year of age (primarily of Dutch or French descent). It can be triggered by infection, stress, or vaccinations.
Symptoms include sudden recurrent attacks lasting 3-7 days, called flares, with other signs like:
- fever
- stomach aches
- rashes
- canker sores in the mouth lining
- swollen lymph nodes
Infection
Certain disorders arise due to infection in young children. Disorders like haemolytic uremic syndrome are an example of this, where children infected with Escherichia coli (E. coli) bacteria develop a disruption in the digestive tract, which causes toxic substances to be allowed into the bloodstream. These substances eventually damage the blood vessels and blood cells. This infection causes vomiting, bloody diarrhoea, and stomach aches in children. Furthermore, haemolytic uremic syndrome in children causes them to become irritable, pale of complexion, and tired. It can eventually lead to kidney failure if left untreated.
Glomerulonephritis is a condition that occurs due to Streptococcus bacterial infection and disrupts the immune system. Excess antibodies, generated as a response to the bacterial infection, collect in a part of the kidney called the glomerulus and eventually damage it. It is curable and, usually, the kidneys can recover from it, but the damage may be permanent in cases where this infection is left untreated.
Nephrotic Syndrome
Nephrotic syndrome is a condition in children where large amounts of a protein, called albumin, are eliminated from the body into the urine. This implies a defect in the kidney filtration process and is a warning sign for kidney damage or failure. This condition is characterised by:
- High protein content in urine (albumin)
- Oedema – swelling of legs, feet, or ankles
- Low levels of albumin protein in the blood
Urine blockage/reflux
These are disorders developed due to the narrowing or obstruction of the tube connecting the kidney and urethra. For instance, posterior urethral valve obstruction results in the reflux of the urine. This means the urine reverses from the bladder back to the kidney. This is because the valve between the bladder and the urethra does not close properly. Doctors can detect it before or just after birth. Other examples include foetal hydronephrosis, which is caused due to damage to the kidneys via conditions like vesicoureteral reflux (VUR). VUR again causes urine reflux from the bladder. Mostly, the doctors need to monitor the patient and perform surgery to remove the obstruction.
Signs of kidney defects in children
Possible signs of kidney defects in children may include low red-blood-cell count (anaemia), bone disease, heart conditions, decreased mental function, nerve damage, susceptibility to infection (due to decreased immune response), and dry and itchy skin. The comparison of acute and chronic kidney diseases are in the following table.
Below: Acute and Chronic Kidney Disease Symptoms in Children
Acute Kidney Disease
- Bleeding (haemorrhage)
- Fever
- Skin rashes
- Diarrhoea with blood
- Vomiting
- Stomach-ache
- Urine imbalance (too much or too less)
- Pale complexion
- Oedema (swelling in body tissues)
- Inflammation around the eye region
- Changes in stomach mass
Chronic Kidney Disease
- Decrease in appetite
- Bone pain and tenderness
- Headaches
- Malaise (discomfort)
- Vomiting
- Issues with hearing
- Urine imbalance and incontinence
- Pale complexion
- Oedema (swelling in body tissues)
- Mouth sores and bad breath
- Changes in stomach mass
- Occurrence of UTIs (urinary tract infection)
- Poor muscle tone
Diagnosis
Urine test
The albumin (protein) content in the urine can be detected by a urine test and can be detected using a chemically treated test strip called the dipstick test. Tests for creatinine, another type of protein, can also be conducted to check for damage caused to the kidneys.
Blood tests
The filtration rate of the kidney can be determined using a blood test and can be analysed to detect defects in kidney function.
Kidney biopsy
This is a method used to closely examine a small chunk of the kidney tissue obtained from the patient's kidneys under the microscope. This technique identifies the extent of damage caused to the kidney in the lab.
Treatment
To treat kidney disorders, the parents should consult a nephrologist and paediatrician. Treatment depends on the symptoms, age, and the overall health of the child.
Below: Acute and Chronic Kidney Disease Treatments in Children
Acute Kidney Disease
- Admission to hospital for treatment
- Intravenous (IV) supply of fluids to compensate for the loss of nutrients from the blood
- Diuretic medication (to increase urine formation by kidneys)
- Monitoring of changes in levels of salts and electrolytes present in the blood
- Dietary changes
Chronic Kidney Disease
- Medication to help with growth and repair of kidney tissues, bone density, and anaemia medication
- Dialysis (artificial blood filtration procedure)
- Diuretic medication (to increase urine formation by kidneys)
- Kidney transplantation, or surgery to prevent kidney failure
- Dietary changes
Dietary changes
Protein
As the kidneys cannot filter waste from protein intake in the diet, limiting the protein intake in the child’s diet is useful. Clinicians may advise what changes need to be made, depending on the severity of the kidney disorder.
Potassium
Due to the risk of hyperkalemia (high potassium levels in the bloodstream), it is advised to reduce the intake of potassium-rich foods in the diet.
Phosphorous
Kidney disorders lead to a build-up of phosphorus in the blood, followed by the elimination of calcium which is essential for bone health, altogether leading to bone-related health problems. Therefore, reduce the child’s intake of phosphorus-rich food.
Sodium
Incorporating a low-sodium diet prevents fluid loss from the body, encouraged by health professionals in the case of kidney disorders.
Lastly, it is highly recommended to consult a healthcare professional in case your child experiences persisting or worsening symptoms or the appearance of new symptoms. Closely monitoring the changes in your child’s health condition and asking about prescribed medication helps to quickly and effectively treat the condition.
References:
- Chaturvedi S, Ng KH, Mammen C. The path to chronic kidney disease following acute kidney injury: a neonatal perspective. Pediatr Nephrol 2017;32:227–41. https://doi.org/10.1007/s00467-015-3298-9




