 Medical contributor:
Medical contributor: First revision:
First revision:  Second revision:
Second revision: MAT: An Introduction
Definition
Multifocal atrial tachycardia (MAT) is a supraventricular (located above the ventricle of the heart) tachycardia (increased heart rate) with an irregular, rapid atrial rhythm arising from multiple ectopic (abnormal location) foci within atria. MAT is one type of arrhythmia (an irregular heartbeat), characterised by a heart rate greater than 100 beats per minute.1
Overview
Multifocal atrial tachycardia is an uncommon arrhythmia seen in elderly patients, usually with underlying conditions. The most common condition associated with MAT is chronic obstructive pulmonary disease (COPD). The pathogenesis of MAT is not well understood; most of the patients are haemodynamically stable and generally asymptomatic. Treatment is based on the treatment of the underlying condition.
Anatomy & physiology
The heart's electrical system
The heart acts as a pump for blood, made up of muscle tissue. The heart needs a source of oxygen and energy to function. The heart's function as a pump is regulated by its electrical conduction system. This system coordinates the contraction of the chambers of the heart. The heart electrical system consists of:
- Sinoatrial node: a small mass of specialized tissue located in the right atria (upper chamber) of the heart (called the sinoatrial node, or SA node)
- Atrioventricular node (AV node)
- Bundle of His: located between right and left ventricle
- Bundle branch: resulting from the division of the bundle of His into right and left
MAT vs. normal heart conduction
Normally, an electrical stimulus is generated by the SA node. In normal conditions, the SA nodes generate an electrical stimulus very regularly, 60 to 100 times per minute. The electrical impulse travels from the SA node to the AV node. The impulses are slowed down for a short period, then continue down via the bundle of His into the ventricle, and then through the bundle branch to stimulate the right and left ventricle. Normally, the heart contracts about 60 to 100 times a minute, depending on a person's age. In MAT, there is an abnormality in the atria that automatically generates an electric stimulus, resulting in an increase in the ability of atrial muscle cells to contract.1
Causes & risk factors
Underlying causes
As mentioned above, MAT is associated with other conditions. The most common cause is COPD. Other causes include: 1
- Pulmonary artery hypertension
- Coronary artery disease
- Acute Respiratory failure
- Congestive heart failure
- Diabetes
- Major surgery
- Drug and Kidney failure
- Electrical abnormality (low levels of magnesium and potassium)
Risk factors
Common risk factors include:
- Lung disease (such as chronic obstructive pulmonary disease and asthma)
- Some drugs (digoxin, theophylline)
- Alcohol, caffeine, cocaine, and amphetamine
Symptoms & signs
Symptoms
MAT can be asymptomatic or present with the symptoms of lung disease or symptoms of another underlying condition. Generally, the symptoms of atrial tachycardia include:2
- Fast heart rate
- Lightheadedness
- Chest pain or pressure
- Shortness of breath
Complications
Persistence of focal atrial tachycardia can result in cardiomyopathy. Which result in symptoms include: 2
- Dyspnea (shortness of breath) with exertion
- Increased lower extremity oedema
- Chest pain
- Risk of sudden cardiac death
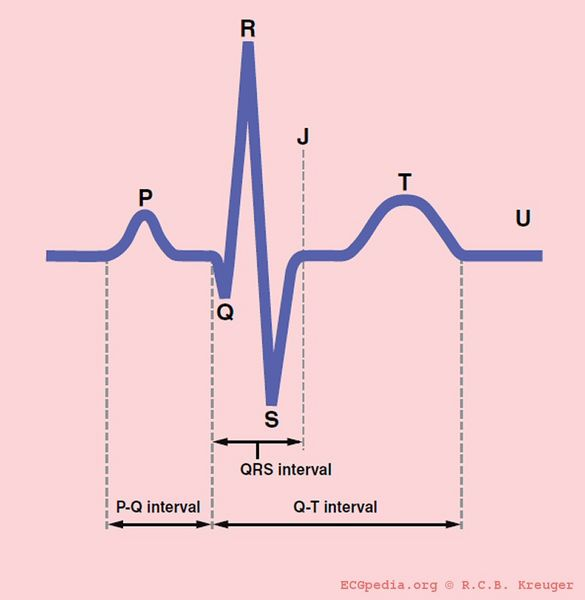
The appearance of MAT on an ECG
An electrocardiogram (ECG) shows irregular rhythms with at least three different P wave morphologies, typically with a gap between them.
Diagnosis
Diagnostic criteria
The role of ECG
Diagnostic criteria for MAT include:
- An irregular heart rate greater than 100 beats per minute
- At least three different P wave morphologic presence of the isoelectric(flat) line between P waves
- Irregular P-wave to P-wave interval
Insert Image: https://commons.wikimedia.org/wiki/Category:ECG_entities#/media/File:De-QRSwaves_(CardioNetworks_ECGpedia).jpg.
Ruling out other tachycardias
To differentiate between MAT and other types of tachycardia, we perform an ECG. An ECG of supraventricular tachycardia usually shows a narrow QRS interval. The morphology (shape) of the P wave also gives an indication of the site and mechanism of the atrial tachycardia.
For atrial tachycardia with long P-to-R interval and short P-R interval, other types include:
- Atypical AVNRTs (atrioventricular nodal re-entry tachycardia), such as fast-slow
- Atrioventricular reentry tachycardia (AVRT) reciprocal junctional tachycardia
- Sinus tachycardia
- Sinus re-entry tachycardia
Atrial tachycardia with short P- R and long P-R intervals – the other types include:
- AVRT
- AVNRT
- Uctional tachycardia
- Trial tachycardia with first-degree AV block
- Atrial tachycardia originating from the coronary sinus ostium
Diagnosis often requires vagal stimulation or adenosine
Other diagnostic tests
In MAT, if the arrhythmia mechanism is an increase in the triggered cardiac activity or automatism, a stress test could be useful to facilitate the induction of the arrhythmia.
Other diagnostic-test include:
- Laboratory studies include a basic metabolic panel, magnesium level, complete blood count, and thyroid-stimulating hormone (TSH) levels.
- A chest X-ray may reveal an enlarged heart (cardiomegaly)
- Echocardiogram to reveal structural heart disease
Treatment & management
Treating underlying conditions
The initial management focused on treating underlying conditions, including:2
- Treating acute illness
- Stress reduction
- Cessation of stimulants
- Chronic disease management
- Appropriately managing digoxin toxicity
Medication
The ventricular contraction rate (heart rate) is controlled using beta blockers or calcium channel blockers. 2 In the absence of underlying pulmonary (lung) disease, the first-line drugs are beta-blockers. Beta-blockers reduce sympathetic stimulation and decrease conduction through the AV node. Most patients did not need beta-blockers as a long-term therapy.1
In the presence of underlying pulmonary disease, the first-line treatment is a non-dihydropyridine calcium channel blocker such as diltiazem or verapamil. These act to decrease conduction through the AV node and suppress the atrial contraction rate. Calcium channel blockers should be avoided in patients with AV blocks, except if the pacemaker has been implanted.1
Electric cardioversion
Cardioversion is the best treatment if the patient is haemodynamically unstable. It is not useful to treat MAT. Electrical cardioversion without concurrent medical therapy can result in arrhythmia recurrence. 2
Long-term therapy
The ventricular contraction rate is controlled by using beta-blockers or calcium channel blockers.2
Prognosis & outcomes
Expected outcomes
Complications
The prognosis depends on the underlying cause. Incessant atrial tachycardia can contribute to reversible heart failure and tachycardic cardiomyopathy. The prognosis of MAT is related to underlying lung disease.
Impact of underlying conditions
As mentioned above, persistent focal atrial tachycardia can result in cardiomyopathy. There is some risk of sudden cardiac death.
Prevention
Lifestyle modifications
Making the following lifestyle changes helps in prevention:
- Avoid caffeinated beverages
- Avoid alcohol
- Quitting tobacco use
- Eating heart-healthy food
- Control blood pressure and cholesterol levels.
Medication and condition management
You can manage it by:1
- Treating the underlying condition
- In the presence of pulmonary disease, the first line of management is calcium channel blockers such as sanitization and verapamil.
- In cases of refractory multifocal atrial tachycardia, AV node ablation has been performed.
- Follow up with your healthcare provider.
Research & future directions
Current research
Recent research has focussed on the treatment of MAT with aprindine. This medication was found to be successful in the treatment of newborns.3
Emerging therapies
In a few studies, parenteral magnesium has proved to decrease the ventricular contraction rate in MAT. Magnesium prevents supraventricular ectopic activities by restoration of ionic equilibrium in atrial heart muscle cells.
In 2017, various electrophysiological invasive approaches were tested for the treatment of MAT, which was resistant to medical therapy.
Summary
Multifocal atrial tachycardia (MAT) is a supraventricular tachycardia (increased heart rate) with an irregular, rapid atrial rhythm arising from multiple ectopic (abnormal location) foci within the atria. MAT is a type of arrhythmia (an irregular heartbeat) characterised by a heart rate that is greater than 100 beats per minute. Diagnosis is done by ECG, and MAT can be asymptomatic. MAT is rated by calcium channel blockers. It can be prevented by lifestyle management.
References
- Custer AM, Yelamanchili VS, Lappin SL. Multifocal atrial tachycardia. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Nov 1]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK459152/
- Liwanag M, Willoughby C. Atrial tachycardia. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Nov 1]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK542235/
- Koroki M, Yokoyama T, Nagara S, Inukai S, Tanaka T. Treatment of multifocal atrial tachycardia with aprindine. Pediatrics International [Internet]. 2020 Jul [cited 2023 Nov 1];62(7):869–70. Available from: https://onlinelibrary.wiley.com/doi/10.1111/ped.14204




