 1st Revision:
1st Revision:  2nd Revision:
2nd Revision: Overview
The term ‘posterior vitreous detachment’ can sound concerning if you’ve never heard it before.
Posterior vitreous detachment (PVD) is a common age-related eye condition in which the vitreous humour detaches from the retina at the back of the eye (hence the name!). It is part of the normal ageing process, but the symptoms can cause distress and affect your ability to carry out your usual activities if your symptoms are particularly bothersome. A posterior vitreous detachment can sometimes precede another eye condition called retinal detachment. Read on to find out more about this condition.
Causes of PVD
First, let’s talk about the eye structures involved in posterior vitreous detachment (Image 1 below).
Image 1: Eye [Internet]. Servier Medical Art. [cited 2023 Jun 16]. Available from: https://smart.servier.com/smart_image/eye/. Modifications: labelled.
The vitreous is a transparent jelly-like substance that gives structure to the eye and helps magnify light rays that enter through the lens. The vitreous makes up around 2/3 of the eye’s size and consists of water, collagen, and hyaluronic acid.1
The retina covers the back of the eye and is packed full of photoreceptors (light receptors) which detect light entering the eye. The retina sends electrical signals to your brain to help translate the light rays into images.2
The vitreous gel is enclosed within the hyaloid membrane. At the back of the eye, where the vitreous meets the retina, this is referred to as the posterior hyaloid membrane. This membrane is made of collagen.
Normally, the vitreous is fully attached to the retina, but as we age, the vitreous loses its structural power and its consistency becomes more watery. The vitreous shrinks and pulls away from the retina—in other words, the vitreous detaches from the retina (Image 2 below).
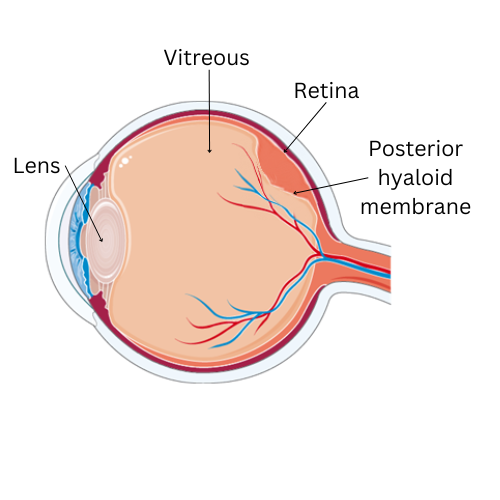
Image 2: Posterior Vitreous Detachment (adapted from Image 1).
This should be a painless process but can result in vision changes as it happens. As the gel degenerates, the collagen inside it can condense and form clumps that cause abnormal shapes (floaters) to appear in the patient’s vision.3 Posterior vitreous detachment does not cause vision loss since the vitreous does not have to be attached to the retina for light signals to be processed into images.
When posterior vitreous detachment progresses rapidly or the vitreous detaches with too much traction, it may tug at the retina and cause a retinal tear. This can further progress into retinal detachment, which is a medical emergency and requires urgent referral to an ophthalmologist (eye doctor). If left untreated, retinal detachment can lead to permanent loss of vision. Posterior vitreous detachment is associated with a specific type of detachment called rhegmatogenous retinal detachment, which occurs when vitreous liquid leaks behind the retina via a tear and causes the retina to detach from its normal position.4 Retinal detachment causes vision loss because the retinal blood supply is disrupted when the retina separates from the back of the eye, causing the retinal tissue to die.
Posterior vitreous detachment can also cause vitreous haemorrhage. This occurs when the vitreous pulls on a blood vessel in the retina and ruptures it.
We’ll explore other features in the ‘Signs and Symptoms’ section.
Risk factors
In most cases, posterior vitreous detachment is a part of the normal ageing process and progresses quickest between the ages of 40 and 70 years old.5 However, posterior vitreous detachment can also be associated with:
- Cataract surgery6
- Myopia (shortsightedness)7
- Previous eye injury
Signs and symptoms of PVD
Posterior vitreous detachment often presents with visual changes. Patients may notice:
- Floaters
- These are often described as dark abnormal moving shapes (lines, specks, dots, cobwebs). Patients may notice them more when looking at a bright background. Blinking doesn’t get rid of them8
- Floaters are caused by light passing through irregularities in the vitreous caused by the change in its consistency1,3
- Flashes of light
- Patients may complain of flashing lights in their peripheral vision. They may be more noticeable in dim settings, or upon head movement9
- Flashes occur when the vitreous separates from the retina, triggering the retina to send a signal to the brain which interprets this signal as a flash of light
- Blurred vision
- The vitreous can pull on and distort the retina, causing blurred vision
- Distortion of central vision
- This is less likely to occur in isolated vitreous detachment
- Central distortion is associated with a macular hole (a tear in a specific region of the retina)
If a patient also has a retinal detachment, they may experience a painless loss of vision or describe a shadow or curtain moving across their vision. If they already have floaters, they may notice a sudden increase in the number or size of floaters or more flashes of light.
Vision loss does not typically occur in posterior vitreous detachment.
Management and treatment for PVD
Once a diagnosis of posterior vitreous detachment has been made, patients usually are followed up in 4-6 weeks to monitor any changes such as the development of a retinal tear or retinal detachment.
There are no treatments to stop, treat, or prevent vitreous detachment, so management is conservative and focuses on symptomatic management.
The eye can adapt to the floaters, making them less intrusive, or the floaters will resolve with no medical or surgical intervention. In some patients, this occurs within six months. However, floaters persist in many patients. They can be mild and cause minimal disturbance, but if floaters are particularly problematic, there are some treatments available to patients.9,10
- Pharmacologic vitreolysis: use of medications to dissolve the proteins in the vitreous
- Laser vitreolysis: laser treatment to destroy vitreous floaters
- Vitrectomy: surgical removal of the vitreous body (eye surgery)
However, there can be side effects associated with these procedures, so the full risks and benefits of each procedure should be carefully weighed to determine the best treatment regimen. Patients should undergo a comprehensive medical review with an ophthalmologist before opting for any procedures. Surgery should be reserved for severe cases which have not responded to other treatments as it is associated with more risk.
If a posterior vitreous detachment has resulted in a retinal tear or retinal detachment, patients may be referred to a retina specialist. A retinal tear may be treated with laser photocoagulation.
Diagnosis of PVD
Patients are usually seen by an ophthalmologist who will perform tests to diagnose the condition. These tests include:
- Dilated eye examination (ophthalmoscopy): eye drops are used to enlarge the pupils to allow the doctor to get a full view of the inside of the eye
- Optical coherence tomography (OCT): allows for visualisation of vitreoretinal surface (does not allow assessment of the entire vitreous)
- B-scan ultrasound: allows the doctor to view structures inside the eye
These investigations will allow the ophthalmologist to rule out other eye conditions which present similarly such as a retinal detachment, central retinal vein occlusion, central retinal artery occlusion, and diabetic retinopathy.
FAQs
How can I prevent PVD?
- PVD cannot be prevented as it is a natural part of the ageing process
- However, it is recommended to note any changes in your vision and seek professional help so that an early diagnosis can be made to reduce significant impact. Early diagnosis can be important in other similarly presenting conditions (e.g., retinal detachment) that have a poor prognosis if treatment is delayed
How common is PVD?
- PVD is present in at least one eye of patients aged 70 and over11
- 5-15% of patients who present with PVD-associated symptoms also have a retinal tear1,12,13
- 3.4-5.2% of patients develop a retinal tear six weeks after a diagnosis of PVD only12,14
When should I see a doctor?
- Ideally, you should see a doctor at your earliest convenience if you notice any changes in your vision
- Changes that may warrant emergency contact include sudden onset loss of vision and the sudden appearance of flashing lights or floaters
Summary
In summary, posterior vitreous detachment is a commonly occurring age-related eye condition that can result in vision changes such as floaters and flashes, which can gradually settle over time. Floaters can persist after six months, but an eye specialist can offer procedures such as laser vitreolysis or surgery to reduce the impact of this symptom.
If you notice any changes in your vision, get in touch with a healthcare professional as soon as possible who may refer you to an ophthalmologist to perform further tests.
References
- Bond-Taylor M, Jakobsson G, Zetterberg M. Posterior vitreous detachment - prevalence of and risk factors for retinal tears. Clin Ophthalmol. 2017;11:1689–95. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5609787/
- Nguyen KH, Patel BC, Tadi P. Anatomy, head and neck: eye retina. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Jun 16]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK542332/
- Mamou J, Wa CA, Yee KMP, Silverman RH, Ketterling JA, Sadun AA, et al. Ultrasound-based quantification of vitreous floaters correlates with contrast sensitivity and quality of life. Invest Ophthalmol Vis Sci. 2015 Jan 22;56(3):1611–7. Available from: https://pubmed.ncbi.nlm.nih.gov/25613948/
- Feltgen N, Walter P. Rhegmatogenous retinal detachment--an ophthalmologic emergency. Dtsch Arztebl Int. 2014 Jan 6;111(1–2):12–21; quiz 22. Available from: https://pubmed.ncbi.nlm.nih.gov/24565273/
- Hayashi K, Sato T, Manabe SI, Hirata A. Sex-related differences in the progression of posterior vitreous detachment with age. Ophthalmol Retina. 2019 Mar;3(3):237–43. Available from: https://pubmed.ncbi.nlm.nih.gov/31014700/
- Ripandelli G, Coppé AM, Parisi V, Olzi D, Scassa C, Chiaravalloti A, et al. Posterior vitreous detachment and retinal detachment after cataract surgery. Ophthalmology. 2007 Apr;114(4):692–7. Available from: https://pubmed.ncbi.nlm.nih.gov/17208303/
- Hayashi K, Manabe SI, Hirata A, Yoshimura K. Posterior vitreous detachment in highly myopic patients. Invest Ophthalmol Vis Sci. 2020 Apr 9;61(4):33. Available from: https://pubmed.ncbi.nlm.nih.gov/32334432/
- Lumi X, Hawlina M, Glavač D, Facskó A, Moe MC, Kaarniranta K, et al. Ageing of the vitreous: From acute onset floaters and flashes to retinal detachment. Ageing Res Rev. 2015 May;21:71–7. Available from: https://pubmed.ncbi.nlm.nih.gov/25841656/
- Ahmed F, Tripathy K. Posterior vitreous detachment. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Jun 16]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK563273/
- Milston R, Madigan MC, Sebag J. Vitreous floaters: Etiology, diagnostics, and management. Surv Ophthalmol. 2016;61(2):211–27. Available from: https://pubmed.ncbi.nlm.nih.gov/26679984/
- Uchino E, Uemura A, Ohba N. Initial stages of posterior vitreous detachment in healthy eyes of older persons evaluated by optical coherence tomography. Arch Ophthalmol. 2001 Oct;119(10):1475–9. Available from: https://pubmed.ncbi.nlm.nih.gov/11594947/
- Hollands H, Johnson D, Brox AC, Almeida D, Simel DL, Sharma S. Acute-onset floaters and flashes: is this patient at risk for retinal detachment? JAMA. 2009 Nov 25;302(20):2243–9. Available from: https://pubmed.ncbi.nlm.nih.gov/19934426/
- Seider MI, Conell C, Melles RB. Complications of acute posterior vitreous detachment. Ophthalmology. 2022 Jan;129(1):67–72. Available from: https://pubmed.ncbi.nlm.nih.gov/34324945/
- van Overdam KA, Bettink-Remeijer MW, Mulder PG, van Meurs JC. Symptoms predictive for the later development of retinal breaks. Arch Ophthalmol. 2001 Oct;119(10):1483–6. Available from: https://pubmed.ncbi.nlm.nih.gov/11594948/




