

Overview
Symbrachydactyly (sim-brack-ee-dack-til-ee) is a rare congenital hand difference – meaning it is present at birth – that affects the development of the fingers or hand. This condition is characterised by short, webbed, or missing fingers: “symbrachydactyly” literally means joined (“sym”), short (“brachy”) fingers (“dactyly”).1
Symbrachydactyly typically affects only one hand (most often the left side), although in 1-7% of cases both hands are affected.2 This condition has diverse morphological forms and clinical presentations vary hugely between individuals. Because of this, symbrachydactyly can often be confused with other types of congenital hand differences, such as amniotic constriction band. However, this condition mostly differs in that the underlying structures of the hand (e.g. the bones, muscles, tendons, ligaments, and nerves) are affected, not just the fingers.
Signs and symptoms of symbrachydactyly
Typical features of symbrachydactyly involve short fingers (brachydactyly), webbed or joined fingers (syndactyly), and small nubs of skin and soft tissue in the place of fingers (“nubbins”) on one hand. However, these symptoms can vary a lot between individuals and symbrachydactyly can be classified into four different types according to the severity of symptoms:2
- Type 1 - Short-finger symbrachydactyly: All four fingers and a relatively normal thumb are present. The fingers might have missing bones (phalanges) and will be noticeably shorter than typical fingers. This is the most common type of symbrachydactyly
- Type 2 - Oligodactylous symbrachydactyly: A thumb and pinky finger are present but the fingers between them are missing. Sometimes referred to as atypical cleft hand
- Type 3 - Monodactylous symbrachydactyly: Only a fully developed thumb is present. The other fingers might be partially developed but missing bones, muscles, or other tissue. These partially formed digits are often referred to as ‘nubbins’
- Type 4 - Adactylous / peromelic symbrachydactyly: There are no fully developed fingers or thumb visible. The nubbins present may or may not have nail remnants
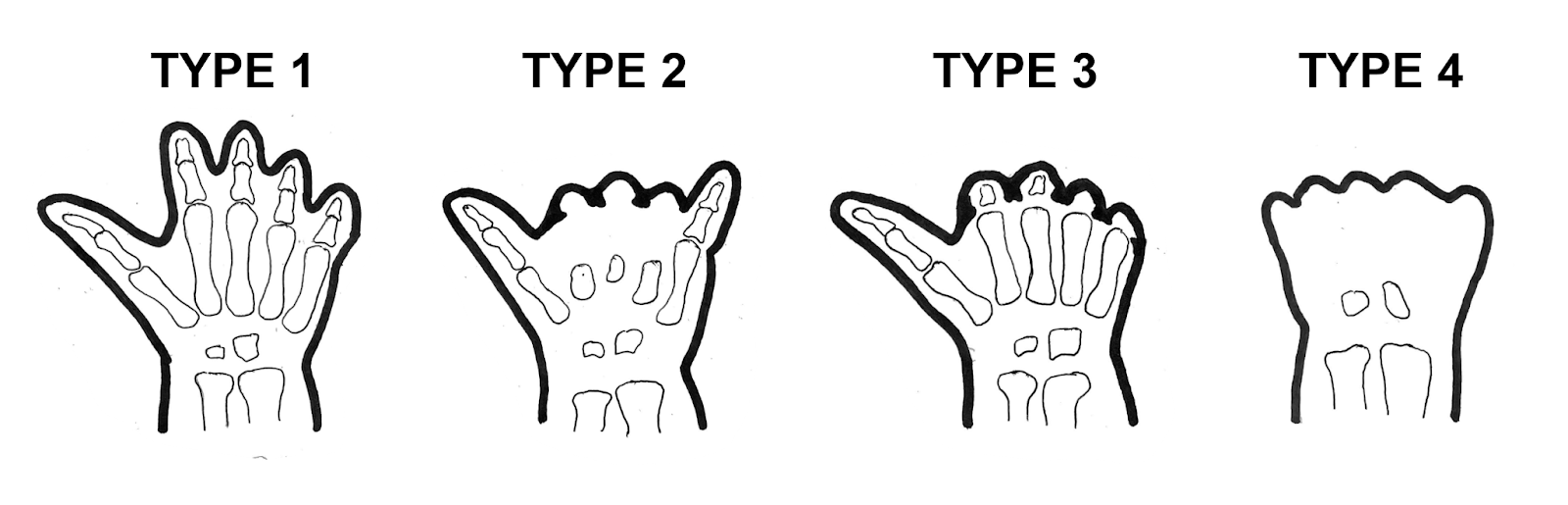
Image Source: Sutherland C.
Causes of symbrachydactyly
The cause of symbrachydactyly is still relatively unknown. There is little evidence of any genetic cause of this condition and it is not thought to be inherited from parent to child.3 This makes symbrachydactyly different from other congenital hand differences, such as polydactyly (extra fingers or toes) or clinodactyly (bending of the fingers), which are typically inherited conditions associated with specific genetic mutations.
During embryonic development in the womb, the hand initially forms in a mitten or paddle shape, before eventually splitting into separate fingers. In babies with symbrachydactyly, the fingers and hand shape generally do not fully form. Experts therefore believe that this condition may be caused by disruption of the blood supply to the developing arm during this development period. However, the actual cause of this disruption is unknown.4
Parents should not feel that they are responsible for causing this hand difference. It is important to realise that there is no link between anything the parents did or did not do during the pregnancy and development of symbrachydactyly.
Diagnosis of symbrachydactyly
Symbrachydactyly can be diagnosed both before birth (prenatal) and after birth (postnatal):
Prenatal diagnosis
Prenatal diagnosis of symbrachydactyly can be made through prenatal ultrasound scans. These tests can visualise the developing limbs of the foetus and might be able to reveal any limb differences, such as undeveloped fingers or missing bones.
Postnatal diagnosis
Most diagnoses of symbrachydactyly are made postnatally. Complicated tests are not normally needed to diagnose symbrachydactyly as you can often visibly see your baby’s affected hand as soon as they are born.
Your healthcare provider will typically conduct a physical examination to identify the characteristic hand features of this condition, although other scans might also be used:
- X-ray to look specifically at the bone structures in the affected hand
- MRI to give a more detailed insight into any soft tissue abnormalities, for example the muscles, tendons, and ligaments in the hand and fingers
Treatment and management of symbrachydactyly
Management of symbrachydactyly typically requires a multidisciplinary approach, often involving surgery, the use of prosthetics, and occupational therapy. Treatment strategies will depend on the severity or type of symbrachydactyly, and are tailored to the specific needs and functional goals of the individual affected.
Surgery
Surgical procedures are a common component of treatment to improve hand function and appearance. There are many different types of surgery, and procedures might involve removal of nubbins, finger lengthening, web space release, or reconstruction of missing fingers. Certain procedures might not be suitable for all individuals depending on the type or severity of symbrachydactyly; your healthcare provider will discuss the options available for your child.5
Surgery is typically performed at different stages of a child’s development to consider their individual needs and growth. Additionally, because symbrachydactyly is mostly unilateral (only affecting one hand), many parents choose to delay surgery and see how the child develops and manages with the condition.
Procedures might include:6
- Syndactyly release: The skin and soft tissue connections (or webbing) between digits are released, resulting in independent fingers to improve function. It is generally advised to do this procedure early in development (as early as 6-12 months old) so that your child’s fingers can grow individually and avoid further shortening of the digits5
- Non-vascularised toe phalanx transfer: A phalanx from a toe (the small bones in your toes) is removed and transferred to an empty finger skin pocket to reconstruct missing fingers or lengthen shortened digits. This procedure is ‘non-vascularised’ which means that the transferred phalanx does not have its own blood supply
- Microvascular toe-to-hand transfer: An entire toe is removed from the foot and transplanted onto the hand to replace a missing finger or thumb to help form a pinch grip. In contrast to the non-vascularised toe phalanx transfer, this procedure involves transplantation of the blood vessels and nerves associated with the toe. This is a complex procedure generally has a success rate over 95%7
- Distraction lengthening: Shortened bones in the hand are lengthened with an external fixator to extend short fingers. This procedure may also be referred to as ‘distraction augmentation manoplasty’ when it is combined with the non-vascular toe phalanx transfer
Prosthetics and orthotics
The use of prosthetics (artificial hands or fingers) and orthotics (brace or splints) can provide valuable support in addition to, or instead of, surgery. These can be used entirely for cosmetic purposes or can be used to enhance hand function and aid in daily activities, for example to help your child hold and grab objects.
These devices should be fitted by a specialist referred to you by your healthcare provider.
Physical and occupational therapy
Rehabilitation and therapy can help your child develop hand skills and adapt to any functional challenges. This might involve:
- Physical therapy to improve the ability of your child to move and use their affected limb.
- Occupational therapy to teach your child how to make best use of their affected hand to perform daily activities and promote independence in their everyday life. These exercises will typically evolve over time to help your child adapt to different tasks as your child grows
Prognosis for those affected by symbrachydactyly
The long-term outlook for individuals with symbrachydactyly is generally positive. Surgery or other treatment options can improve the function and appearance of the affected hand and many people can live their lives unaffected by their hand difference.
However, some functional limitations will likely remain which could affect some aspects of daily life. These limitations will vary between individuals based on the severity or type of their condition and their response to treatment. Ongoing medical management is often required to monitor growth and address any changes or complications that might arise.
FAQs
How common is symbrachydactyly?
Symbrachydactyly is a rare congenital hand difference, with around 1 in 32,000 babies born with this condition.
Are there risks of symbrachydactyly surgery?
Complications after surgery are uncommon and usually minor, but risks do exist. These complications might include infections, poor bone healing, stiff knuckle joints, or finger dislocation.6
What is the difference between symbrachydactyly and brachydactyly?
Symbrachydactyly and brachydactyly are both terms related to congenital limb differences, but they refer to different conditions with distinct characteristics. Symbrachydactyly is a hand difference characterised by shortened and webbed fingers or missing digits typically only affecting one hand. In contrast, brachydactyly refers to a group of congenital limb differences affecting both the hands and/or feet, resulting in shortened fingers or toes.
What is Poland’s syndrome and symbrachydactyly?
Poland’s syndrome is another rare congenital disorder which primarily affects the chest, causing underdeveloped or missing chest muscle on one side of the body. However, some individuals with Poland’s syndrome also display hand differences characteristic of symbrachydactyly, and symbrachydactyly was first described in patients with Poland’s syndrome by Poland in 1841.1
Summary
To summarize, symbrachydactyly is a rare congenital condition that affects the development of the hand and fingers. Symptoms include short fingers that are typically webbed or joined and small nubs of skin and soft tissue in the place of fingers, although the severity of these symptoms varies between individuals. Typically, only one hand is affected. The exact cause of this condition is unknown but there is no evidence for a genetic cause and it is not thought to be passed on from parents to their children. This condition can have a significant impact on individuals and their families, but with comprehensive treatment and ongoing support many individuals can lead fulfilling lives.
References
- Goodell PB, Bauer AS, Sierra FJA, James MA. Symbrachydactyly. Hand (N Y) [Internet]. 2016 Sep [cited 2023 Nov 8];11(3):262–70. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5030846/
- Woodside JC, Light TR. Symbrachydactyly — diagnosis, function, and treatment. The Journal of Hand Surgery [Internet]. 2016 Jan [cited 2023 Nov 8];41(1):135–43. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0363502315008291
- Dahl WJ, Jones NF. Symbrachydactyly. In: Laub Jr. DR, editor. Congenital Anomalies of the Upper Extremity: Etiology and Management [Internet]. Cham: Springer International Publishing; 2021 [cited 2023 Nov 8]. p. 177–204. Available from: https://doi.org/10.1007/978-3-030-64159-7_12
- Mills JK, Butler L, Mills EM, Oishi SN. Symbrachydactyly: Finger nubbins are not always amniotic band disruption sequence. JAAPA [Internet]. 2019 Apr [cited 2023 Nov 8];32(4):32. Available from: https://journals.lww.com/jaapa/abstract/2019/04000/symbrachydactyly__finger_nubbins_are_not_always.6.aspx
- Balakrishnan G, Vijayaragavan S, Somesh B. Symbrachydactyly. Indian J Plast Surg [Internet]. 2022 Feb [cited 2023 Nov 8];55(1):7–17. Available from: http://www.thieme-connect.de/DOI/DOI?10.1055/s-0041-1734579
- Bartsch A, Nikkhah D, Miller R, Mende K, Kaempfen A. Correction of Symbrachydactyly A systematic review of surgical options [Internet]. In Review; 2023 Feb [cited 2023 Nov 8]. Available from: https://www.researchsquare.com/article/rs-2316285/v1
- Jones NF, Hansen SL, Bates SJ. Toe-to-hand transfers for congenital anomalies of the hand. Hand Clinics [Internet]. 2007 Feb 1 [cited 2023 Nov 8];23(1):129–36. Available from: https://www.sciencedirect.com/science/article/pii/S0749071207000169




