

Introduction
In medicine, signs can be used to identify symptoms that might be suggestive of an underlying problem, often based on a bodily response to a test. One such example is Tinel’s sign, which is characterised by a tingling sensation, pins and needles, or pain when the skin covering a nerve is touched. This is indicative of conditions such as carpal tunnel syndrome, or trapped or compressed nerves, and can even be used to monitor nerve damage after an injury.1
Tinel’s sign is eponymously named after a French neurologist, Dr Jules Tinel who served as a military doctor during the First World War. Dr Tinel studied and treated cases of nerve damage caused in combat in the years following the war, which led to his discovery of Tinel’s sign. He is credited with huge contributions to the field of neurology through his published works, the most famous of which was published in 1916.1,2
It has been noted, however, that while his research was extensive, Tinel was not the first neurologist to report the phenomenon of Tinel’s sign. Therefore, the sign is sometimes referred to as the Hoffman-Tinel sign to credit the German neurologist who wrote about the sign even before Tinel did.1,2
Anatomy and physiology
Nerves enable the rapid transmission of signals around the body. The nervous system is complex, and is made up of the central nervous system: the brain and the spinal cord, and the peripheral nervous system, which is an extensive network of nerves throughout the body. Disease, traumatic injury or genetic conditions can result in damage to these peripheral nerves.3 For example, this can occur through damage to neighbouring blood vessels, cutting off oxygen supply, toxin damage, partial or total severing of the nerve, compression of the nerve, or autoimmune diseases attacking the nerves.4,5
Damage to nerves can result in disruption to the signals that the nerves deliver and can also manifest with symptoms such as pain, numbness, and tingling.3
The body can regenerate damaged nerve cells, although this process of regeneration is not as quick or as comprehensive as the regeneration of other cells, like skin cells or muscle cells.
Mechanism of Tinel's sign
A positive result for Tinel’s sign is characterised by tingling, pins and needles or even sharp shooting pains when the skin is tapped gently along the pathway of the nerve. A positive Tinel’s sign is indicative of nerve damage and regeneration. This is because damaged, pinched or compressed nerves are stimulated at the point of the tap, and become irritated, sending abnormal signals which result in the tingling, pain or pins and needles associated with a positive Tinel’s sign.6
There are different types of nerve damage that Tinel’s sign can detect.
Nerve compression
Nerve compression occurs when the nerve is pinched or squeezed between other structures. Tapping the skin over the area of nerve compression can stimulate the nerve, resulting in a positive Tinel’s sign. 6
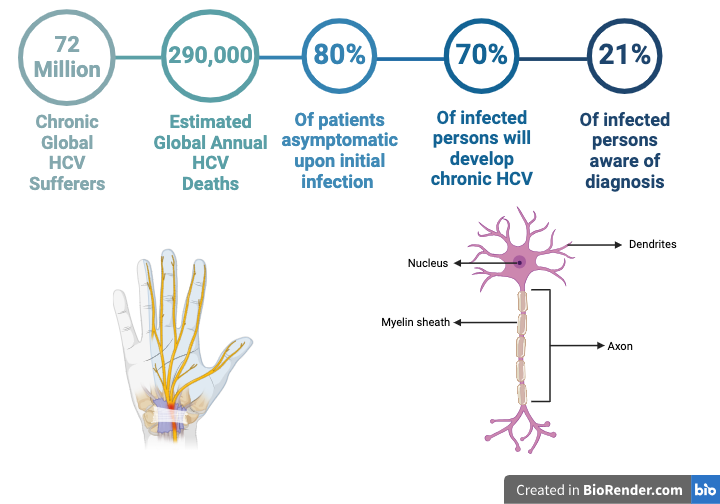
Figure 1: Basic Nerve Cell - Created by the author using Biorender.com.
Axonal degeneration
Axonal degeneration is another type of nerve damage that results in a positive Tinel’s sign. Axonal degeneration is where the axon, the long fibre of the nerve which conducts the signal along it, as seen in Figure 1, begins to degenerate.7 This commonly occurs after the nerve cell has sustained some damage, whether through injury, genetic conditions, infections, toxin exposure, diseases such as HIV, diabetes or hepatitis, or a reduced blood supply.7 Once this damage occurs, the axon of the nerve will begin to degenerate, disrupting the signal. This type of degeneration may lead to a positive Tinel’s sign as tapping the skin over the area of nerve damage causes the remaining and intact axons in the area to send signals, which can result in tingling or pain.8
Wallerian degeneration
Finally, Wallerian degeneration is a complex way in which the body tries to degenerate and clear away damaged nerves. Wallerian degeneration typically occurs after a nerve cell is severely damaged or severed. This could be through surgery, or a severe injury. This will cause the axon to degenerate9,10 but leave the rest of the cell alive. The immune system then clears away the degenerated nerve cell parts, which gives the body space and resources to begin to regenerate the damaged axon, although this is a slow and imperfect process.11 The severity and location of the injury, and age, health and damage to the individual and the surrounding tissues will determine the extent of the possible regeneration.12 Wallerian degeneration can be less reliably identified by a positive Tinel’s sign, as if the nerves are severed, they may not be able to transmit any signals which are required to cause the characteristic symptoms of a positive sign. However, conducting the test further away from the site of injury may still give a positive Tinel’s sign if the nerve cells in the area have been irritated or inflamed by the injury.
Clinical significance
Tinel’s sign has been linked to multiple conditions. The main conditions associated with Tinel’s sign are carpal tunnel syndrome, cubital tunnel syndrome, tarsal tunnel syndrome, as well as some nerve injuries. Let’s take a look at the clinical significance of Tinel’s sign with respect to each of these conditions.
Carpal tunnel syndrome
Carpal tunnel syndrome is the most common condition associated with a positive Tinel’s sign. This condition happens when the carpal tunnel, which the nerve runs through, becomes narrowed, causing compression, irritation and inflammation of the median nerve, as seen in Figure 2.13 As mentioned, tapping along the median nerve in the area of injury could therefore irritate the nerve, causing a positive Tinel’s sign.
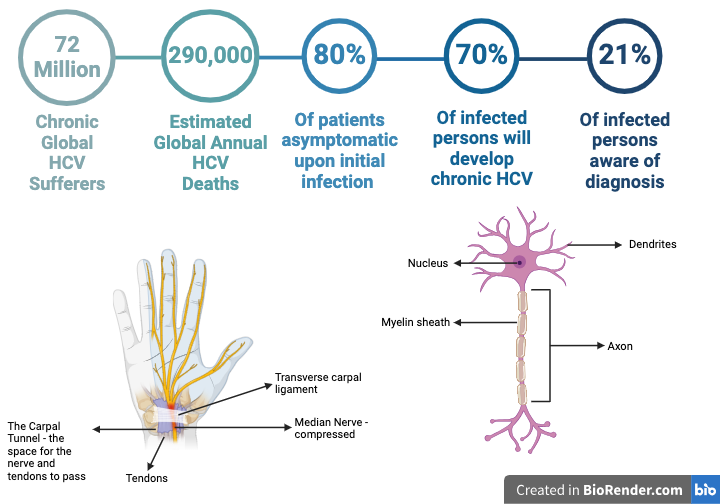
Figure 2: Carpal Tunnel syndrome. Created by the author using Biorender.com.
Cubital and tarsal tunnel syndrome
Cubital tunnel syndrome and tarsal tunnel syndrome, similarly to carpal tunnel syndrome, refer to the compression and irritation of the nerve as it moves through a canal. In cubital tunnel syndrome, however, it is the ulnar nerve that is being compressed at the elbow as it moves through the cubital tunnel causing tingling, pain and numbness into the forearm and ring and little fingers.13 Tarsal tunnel syndrome is the compression of the posterior tibial nerve in the ankle causing tingling and pain in the foot and ankle.14 These, similarly to carpal tunnel syndrome, can cause positive Tinel’s signs as stimulation of the compressed or damaged nerve by tapping the skin can result in tingling or pain - the classic positive Tinel’s sign.
The radial nerve runs down the back of the arm from the armpit into the hand, the sciatic nerve runs through the thigh and buttocks, and the peroneal nerve runs from the knee into the lower leg. Damage or compression of all of these nerves are commonly diagnosed by a positive Tinel’s test.15,16,17
Injuries such as nerve damage and scarring after surgery, nerves in the process of regenerating and nerves being compressed by tumours and malignancies have all been associated with a positive Tinel’s sign.18
Limitations and considerations
Tinel’s sign can be a useful and non-invasive tool to assess potential injury and clinical conditions, however it is just one piece of the puzzle, and shouldn’t be used as the sole diagnostic tool. This is because it does have some limitations.
If nerve damage is severe enough that signals are completely disrupted, tingling, pins and needles and pain may not be felt as the nerve is too damaged to carry signals.19 On the other hand, the nerve damage may also be minimal, meaning that tapping the skin is not sufficient to irritate or stimulate the nerve to tingle or cause discomfort. These problems may lead to false negative results.
In contrast, false positives are also possible, where variations between individuals may cause some nerves to be more easy to stimulate by tapping on the skin, and could cause tingling feelings even in the absence of nerve damage. Other factors, such as healthcare professionals tapping the skin too hard, could also cause tingling or pain.20
Other investigations
As we have seen above, Tinel’s sign is not completely accurate as a diagnostic test alone. Therefore, it is often combined with other tests to form a more comprehensive overview of the condition and symptoms before a diagnosis.
For example, carpal tunnel syndrome is often also diagnosed with Phalen’s test, which involes pressing the hands together at the chest, with the forearms horizonatal and wrists extended. If there is pain, this is a positive sign indicative of carpal tunnel syndrome.19 There are other similar mobility tests for nerve compression injuries which can elicit pain if the nerve is damaged or trapped. When used in conjunction with a detailed medical history and a good understanding of symptoms, medical professionals can gain a good understanding of underlying problems.
Additionally, when assessing nerve damage and its severity, some imaging tools can be effective diagnostic tools. This may include X-rays, MRI scans and CT scans. Nerve conduction tests can also test nerve function and determine the site and extent of damage.
Treatment
Many conditions pertaining to nerve damage can initially be managed at home or conservatively. Limiting activity, repetitive movements, and heavy lifting, all of which exacerbate the problem, is a good starting point. Splints and braces which immobilise joints where nerves are compressed are commonly recommended, especially during sleeping hours, to alleviate pressure on the nerve and manage the pain. Physiotherapists can recommend some exercises which help to maximise mobility to use a full range of motion and limit compression where possible. Anti-inflammatory medications can be used to reduce swelling in the area and alleviate the compression and irritation of the nerve.21
If these strategies fail to manage the problem, corrective surgery is available. Surgical options may be able to release pressure on the nerve in carpal tunnel, cubital tunnel and tarsal tunnel syndromes, as well asr other underlying causes of nerve compression and irritation.
Prognosis and recovery
Nerve damage can be a lengthy and tricky problem for the body to solve on its own. Regenerating damaged nerve tissue is dependent on how severe the nerve damage is, the age and health of the patient, other underlying conditions, and how quickly interventions are available.12 If interventions, medication and corrective surgery occur quickly in an otherwise healthy patient who has been completing physiotherapy exercises and resting, the prognosis is much more positive than for an elderly patient experiencing severe nerve damage from a traumatic injury who has other comorbidities that may make healing more difficult. It is incredibly difficult to predict long-term outcomes for nerve injuries.12
Summary
Tinel’s sign is a useful non-invasive diagnostic tool for healthcare professionals to assess certain conditions associated with nerve damage. Although it may be inaccurate as a sole diagnostic tool, it can be useful when used in conjunction with other tests. Nerve conduction tests, CT scans and MRI scans are all useful tools for assessing and diagnosing suspected nerve damage, but critical research is ongoing into the regeneration of the nervous system, which can be a slow and unreliable process.
References
- Davis EN, Chung KC. The tinel sign: a historical perspective. Plastic and Reconstructive Surgery [Internet]. 2004 Aug [cited 2023 Oct 11];114(2):494. Available from: https://journals.lww.com/plasreconsurg/abstract/2004/08000/the_tinel_sign__a_historical_perspective.31.aspx
- Sansone JM, Gatzke AM, Aslinia F, Rolak LA, Yale SH. Jules tinel (1879–1952) and paul hoffmann(1884–1962). Clin Med Res [Internet]. 2006 Mar 1 [cited 2023 Oct 11];4(1):85–9. Available from: http://www.clinmedres.org/content/4/1/85
- Rotshenker S. Chapter 39 - traumatic injury to peripheral nerves. In: Tubbs RS, Rizk E, Shoja MM, Loukas M, Barbaro N, Spinner RJ, editors. Nerves and Nerve Injuries [Internet]. San Diego: Academic Press; 2015 [cited 2023 Oct 11]. p. 611–28. Available from: https://www.sciencedirect.com/science/article/pii/B9780128026533000889
- Menorca RMG, Fussell TS, Elfar JC. Peripheral nerve trauma: mechanisms of injury and recovery. Hand Clin [Internet]. 2013 Aug [cited 2023 Oct 11];29(3):317–30. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4408553/
- Popoff MR, Poulain B. Bacterial toxins and the nervous system: neurotoxins and multipotential toxins interacting with neuronal cells. Toxins [Internet]. 2010 Apr [cited 2023 Oct 11];2(4):683–737. Available from: https://www.mdpi.com/2072-6651/2/4/683
- Sharrak S, M Das J. Hand nerve compression syndromes. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Oct 11]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK547683/
- Cashman CR, Höke A. Mechanisms of distal axonal degeneration in peripheral neuropathies. Neuroscience Letters [Internet]. 2015 Jun 2 [cited 2023 Oct 11];596:33–50. Available from: https://www.sciencedirect.com/science/article/pii/S0304394015000610
- Tinel sign - an overview | sciencedirect topics [Internet]. [cited 2023 Oct 11]. Available from: https://www.sciencedirect.com/topics/neuroscience/tinel-sign#:~:text=Tinel%20sign%20is%20elicited%20by,cutaneous%20distribution%20of%20the%20nerve.
- Koeppen AH. Wallerian degeneration: history and clinical significance. Journal of the Neurological Sciences [Internet]. 2004 May [cited 2023 Oct 11];220(1–2):115–7. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0022510X04000759
- Conforti L, Gilley J, Coleman MP. Wallerian degeneration: an emerging axon death pathway linking injury and disease. Nat Rev Neurosci [Internet]. 2014 Jun [cited 2023 Oct 11];15(6):394–409. Available from: https://www.nature.com/articles/nrn3680
- Dubový P. Wallerian degeneration and peripheral nerve conditions for both axonal regeneration and neuropathic pain induction. Annals of Anatomy - Anatomischer Anzeiger [Internet]. 2011 Jul 1 [cited 2023 Oct 11];193(4):267–75. Available from: https://www.sciencedirect.com/science/article/pii/S0940960211000537
- Ferrante MA. The assessment and management of peripheral nerve trauma. Curr Treat Options Neurol [Internet]. 2018 Jun 1 [cited 2023 Oct 11];20(7):25. Available from: https://doi.org/10.1007/s11940-018-0507-4
- Thatte MR, Mansukhani KA. Compressive neuropathy in the upper limb. Indian J Plast Surg [Internet]. 2011 [cited 2023 Oct 11];44(2):283–97. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3193641/
- Ahmad M, Tsang K, Mackenney PJ, Adedapo AO. Tarsal tunnel syndrome: A literature review. Foot and Ankle Surgery [Internet]. 2012 Sep 1 [cited 2023 Oct 11];18(3):149–52. Available from: https://www.sciencedirect.com/science/article/pii/S1268773111001226
- Ljungquist KL, Martineau P, Allan C. Radial nerve injuries. The Journal of Hand Surgery [Internet]. 2015 Jan 1 [cited 2023 Oct 11];40(1):166–72. Available from: https://www.sciencedirect.com/science/article/pii/S0363502314006261
- Elvey RL. Physical evaluation of the peripheral nervous system in disorders of pain and dysfunction. Journal of Hand Therapy [Internet]. 1997 Apr 1 [cited 2023 Oct 11];10(2):122–9. Available from: https://www.sciencedirect.com/science/article/pii/S089411309780066X
- Preston D. Iatrogenic needle-induced peroneal neuropathy in the foot. Ann Intern Med [Internet]. 1988 Dec 1 [cited 2023 Oct 11];109(11):921. Available from: http://annals.org/article.aspx?doi=10.7326/0003-4819-109-11-921
- Gosk J, Gutkowska O, Mazurek P, Koszewicz M, Ziółkowski P. Peripheral nerve tumours: 30-year experience in the surgical treatment. Neurosurg Rev [Internet]. 2015 Jul 1 [cited 2023 Oct 11];38(3):511–21. Available from: https://doi.org/10.1007/s10143-015-0620-8
- Ho T, Braza ME. Hoffmann tinel sign. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Oct 11]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK555934/
- Monsivais JJ, Sun Y. Tinel’s sign or percussion test? Developing a better method of evoking a Tinel’s sign. J South Orthop Assoc. 1997 Jan 1;6(3):186–9.
- Piazzini DB, Aprile I, Ferrara PE, Bertolini C, Tonali P, Maggi L, et al. A systematic review of conservative treatment of carpal tunnel syndrome. Clin Rehabil [Internet]. 2007 Apr [cited 2023 Oct 11];21(4):299–314. Available from: http://journals.sagepub.com/doi/10.1177/0269215507077294




