

Wheezing is a high-pitched, whistling sound made when breathing in or out, associated with shortness of breath. This occurs due to narrowed, obstructed airways, commonly experienced by people with asthma. Wheezing can also be caused by a physical obstruction in the airways, and other health issues such as pneumonia and heart failure.
Introduction
Wheezing is a whistling noise caused by restricted airways. This may be accompanied by a feeling of tightness in the chest, difficulty catching your breath, and coughing. Wheezing is often associated with an asthma attack, though not always. Wheezing and asthma are diverse and heterogeneous, meaning that they can occur differently in different patients; no single explanation accounts for all kinds of wheezing.
Biology of wheezing
Physiology of breathing
Before examining what causes wheezing, it is useful to understand what is involved in healthy breathing. In the lungs, an exchange of gas occurs between the air we inhale and the gases that is carried in our bloodstream. When we breathe in, our diaphragm and external intercostal muscles in the ribs contract, creating a larger space in our chest. Air is drawn into the lungs, and oxygen is exchanged for carbon dioxide. When we breathe out, the diaphragm relaxes, and air passively leaves the lungs. If we want to exhale air faster, for example, exercising or singing, we can use the internal intercostal muscles to push air out faster.
“The airways” refers to the tubes that air moves through, also called the respiratory tract. The upper respiratory tract consists of the nasal cavity, where air enters the nose, the pharynx (throat) and larynx (voice box). The lower respiratory tract is the trachea and bronchi, leading into the lungs. The bronchi branch off into smaller tubes in the lungs, called bronchioles, which end at the alveoli, the tiny air sacs where gas exchange occurs.(1)
The airways are lined with smooth muscle, which contracts and relaxes to control the size of the airways and the flow of air. The outer layer or epithelium of the airways contains hair-like ciliary cells and secretory cells which produce mucus. Mucus helps protect the lungs by trapping toxins and dirt, which can then be pushed away from the lungs by the cilia, as well as coughed out in phlegm.
Physiology of wheezing
Wheezing occurs when the airways are inflamed or obstructed. This is called bronchoconstriction when the smooth muscle of the bronchi and bronchioles in the lower respiratory tract contract. As the air flows through the narrowed airway, a musical whistling sound may be heard whilst the almost closed airway walls oscillate and vibrate. Wheezing is heard most during expiration (breathing out) as this is when airways are narrowest, but it can also be heard when breathing in through inspiration if the tightening is severe.2
Wheezing reduces the efficiency of gas exchange in the lungs, therefore, when severe this can result in low oxygen in the blood, insufficient oxygen levels in tissues around the body, and high carbon dioxide in the blood. This causes a feeling of shortness of breath (called dyspnoea), dizziness, confusion and headache.
The role of mucus
During wheezing there is an increase in mucus production, contributing to the narrowed airways. Large proteins called ‘mucins’ are produced by genes expressed in the airways, which help form the protective mucus gel layer along with water, other proteins and ions. Excessive production of mucous can gradually block the flow of air through the airways. When inflammatory pathways are triggered, for example, by allergens, genes such as MUC5AC become overactive and produce more mucous than usual, affecting airflow. Mucus blocking the airways can be a cause of death during a severe asthma attack. (3)
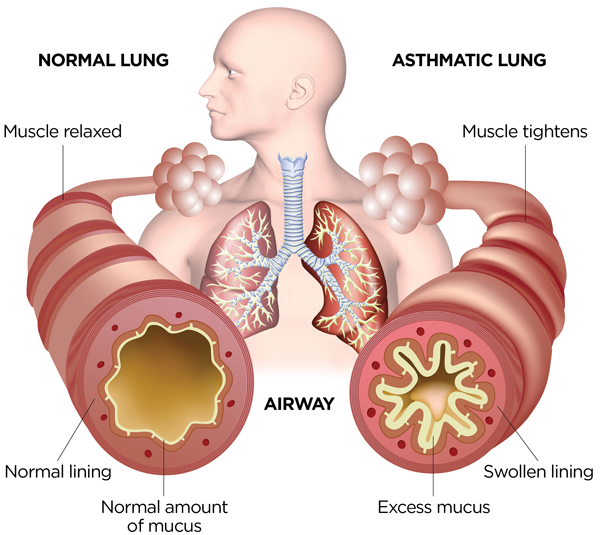
Figure 1: Airways in normal breathing compared to airways during asthma. Ref: Asthma and Allergy Foundation of America.4
Oxidative stress
Triggers of wheezing, such as pollutants and allergens, are found to increase levels of reactive oxygen species, which cause cell damage and death through ‘oxidative stress’. Reactive oxygen species include negatively charged oxygen, O2•− and hydroxyl •OH, which then react with molecules in cells, such as DNA. DNA damage activates DNA repair pathways, triggering further inflammatory signals, which have been found to increase mucus production, leading to smooth muscle in the airways contracting and tightening.5
The role of eosinophils
Eosinophils are a type of white blood cell that carry out immune functions such as fighting fungal infections and defending against parasites. These white blood cells build up in asthma when the airways are inflamed, and the severity of eosinophil accumulation is linked to the severity of asthma (6). Eosinophils secrete inflammatory chemicals, contributing to swelling and mucus secretion. Eosinophils have been explored as a possible biomarker for the diagnosis of some types of asthma as well as a target for treatment. Monoclonal antibody therapies, which specifically target parts of eosinophils, have shown some success in improving lung function and reducing asthma exacerbations, although more research is needed to develop these treatments.6,7
Histamines
Histamine is a chemical released in the body in response to allergens. Mast cells are another type of white blood cell. These release histamine and mediate allergic reactions, causing inflammation and swelling. Samples of fluid from the lung show histamine is increased in asthmatics compared to non-asthmatics.8,9 When triggered by an allergen, histamine receptor H1 causes the contraction of the airway muscles, resulting in reduced airflow and wheezing (8). Histamine is also found to increase mucus production via the receptor H2. Asthmatic patients have ‘hyperresponsive’ airways which overreact to low doses of histamine, which would not affect a non-asthmatic, causing bronchoconstriction.8 As well as causing airway muscle contraction, histamine increases mucus production and causes airway submucosal edema, where the layer of airway below the mucus layer swells, reducing the airway diameter.
Another histamine receptor, H4, increases the movement of eosinophils and activates mast cells which secrete further histamine, amplifying allergic and inflammatory responses.
Treatments targeting histamine receptors appear to be effective in treating some allergic asthma subtypes.8
Immunoglobulin E (IgE)
Immunoglobulin E (IgE) is an antibody linked to allergic reactions. Patients with allergies, allergic asthma, and autoimmune conditions show high IgE levels in their blood. This molecule can be used in the diagnosis of allergic asthma. When exposed to allergens, the immune system produces high levels of IgE to trigger the allergic reaction. Monoclonal antibody treatments targeting IgE are also being explored as another treatment for allergic asthma.10
Absence of wheezing: silent chest
Sometimes in severe asthma, wheezing cannot be heard despite the inflammation of the airways. If the patient feels exhausted because they are struggling to breathe but with no wheeze, this could show that the airways are so severely inflamed that their respiratory system is failing. This is called status asthmaticus and needs immediate treatment.2
Causes of wheezing
Asthma
Asthma is a ‘chronic inflammatory disorder’, meaning that it is a long-term condition involving the activation of immune cells and swelling. There are several different types of asthma.
Allergic or extrinsic asthma
Extrinsic asthma occurs when something ‘foreign’ to the body triggers an allergic reaction, resulting in wheezing or inability to breathe. This is the most common form of asthma, accounting for 80% of childhood asthma and over 50% of all asthma cases.11,12 Extrinsic asthma can be diagnosed by IgE levels. Its onset is often in childhood, starting from 2 years onwards, coinciding with other allergic conditions such as rhinitis (runny nose) and atopic dermatitis or eczema. Allergic asthma is more common in males than females and typically persists into adulthood. Several genes are associated with allergic asthma risk.11
Intrinsic asthma
Intrinsic asthma is non-allergic, mainly occurring in adulthood, past 30 years old. Intrinsic asthma can occur following a respiratory infection, resulting in hyperreactivity to triggers such as cold air, smoke, further infections, and stress.2 Females are more at risk of intrinsic asthma.13
Exercise-induced asthma
For most asthmatics, exercises such as running and cycling can result in wheezing and dyspnea (struggling to breathe) shortly afterwards. The severity of exercise-induced asthma may depend on other factors such as cold or dry air, the type of exercise, and the fitness of the patient.
Asthmatic bronchitis
Asthmatic bronchitis involves chronic (long-term) excess mucus in the airways and hyperreactivity of airway muscles. This is common in elderly cigarette smokers. This is unrelated to allergies.2
Chronic obstructive pulmonary disease (COPD)
COPD is a lung condition including emphysema (damage to alveoli inside the lungs) and bronchitis (long-term inflammation of the airways). The key symptoms of COPD are wheezing, a chesty cough, shortness of breath and frequent chest infections. COPD symptoms are more constant than asthma. COPD mainly affects middle-aged adults who smoke. It can also be caused by long-term exposure to other airway irritants, such as dust or toxic fumes. The treatments include stopping smoking, exercise programmes and inhaled medications to reduce bronchoconstriction.14
Bronchiolitis
This is a common lung infection in young children, where the bronchioles swell and produce excess mucus. Bronchiolitis is often a complication after the common cold or the flu. Children may breathe quickly and develop a fever as well as producing an audible wheezing.
Other triggers
Wheezing may be triggered by viral infections affecting the lungs and airways, such as the flu, or Covid-19. These viruses increase mucus production and activate airway inflammation.
Other irritants may include sudden temperature changes, very dry air, smoke or dust. Physical obstructions in the airway cause wheezing - in this case, the patient would also have coughing and choking symptoms. Some medications can induce wheezing, such as propranolol (beta-blocker prescribed for heart issues and anxiety), aspirin, and some cholinergic drugs.(2)
Treatment for wheezing
The main treatments offered for wheezing are blue reliever inhalers and brown preventer inhalers.15
Reliever inhalers commonly contain salbutamol, which activates β2 receptors to relax smooth muscle and reduce bronchoconstriction. This acts quickly and wears off quickly.
Preventer inhalers commonly contain beclometasone dipropionate, a corticosteroid that reduces the immune response and inflammation in the respiratory system.
There are also long-action drugs that activate β2 receptors for around 12 hours, such as salmeterol and formoterol. These may be prescribed as part of a combination inhaler which both relieves bronchoconstriction and provides a steroid to reduce inflammation in the longer term.
Depending on the cause of the wheezing, other treatments may be required. For example, antibiotics may be given to treat a chest infection. Stopping smoking and exposure to triggers can reduce wheezing.
Modern treatments are also being explored as mentioned earlier in this article: drugs can specifically target mucus production, white blood cells such as eosinophils, histamine receptors or IgE antibodies.
Summary
The causes of wheezing are varied and complex, involving increased mucus in the airways, swelling, and contraction of muscles surrounding the airways. Most commonly, wheezing is an allergic reaction. However, there are several different types with different biological processes behind them. These include oxidative stress, white blood cell accumulation, excess mucus, and the constriction of the airways. Wheezing can be treated effectively using inhalers. Scientists are continuing to advance our understanding of the processes and trialling new treatment options.
References
- Ball M, Hossain M, Padalia D. Anatomy, airway. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan. PMID: 29083624.
- Gong H JR.. Wheezing and Asthma. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. Boston: Butterworths; 1990. Chapter 37. Available from: https://www.ncbi.nlm.nih.gov/books/NBK358/
- Evans CM, Kim K, Tuvim MJ, Dickey BF. Mucus hypersecretion in asthma: causes and effects. Current opinion in pulmonary medicine. 2009 Jan;15(1):4.
- Asthma and Allergy Foundation of America Blog: What happens when you have asthma? https://community.aafa.org/blog/what-happens-in-your-airways-when-you-have-asthma
- Bacsi A, Pan L, Ba X, Boldogh I. Pathophysiology of bronchoconstriction: role of oxidatively damaged DNA repair. Current opinion in allergy and clinical immunology. 2016 Feb;16(1):59.
- Choi BS. Eosinophils and childhood asthma. Clinical and Experimental Pediatrics. 2021 Feb;64(2):60.
- Haldar P, Brightling CE, Hargadon B, Gupta S, Monteiro W, Sousa A, Marshall RP, Bradding P, Green RH, Wardlaw AJ, Pavord ID. Mepolizumab and exacerbations of refractory eosinophilic asthma. New England Journal of Medicine. 2009 Mar 5;360(10):973-84.
- Yamauchi K, Ogasawara M. The role of histamine in the pathophysiology of asthma and the clinical efficacy of antihistamines in asthma therapy. International journal of molecular sciences. 2019 Apr 8;20(7):1733.
- Casale TB, Wood D, Richerson HB, Trapp S, Metzger WJ, Zavala D, Hunninghake GW. Elevated bronchoalveolar lavage fluid histamine levels in allergic asthmatics are associated with methacholine bronchial hyperresponsiveness. The Journal of clinical investigation. 1987 Apr 1;79(4):1197-203.
- Owen CE. Immunoglobulin E: role in asthma and allergic disease: lessons from the clinic. Pharmacology & therapeutics. 2007 Jan 1;113(1):121-33.
- Akar-Ghibril N, Casale T, Custovic A, Phipatanakul W. Allergic endotypes and phenotypes of asthma. The Journal of Allergy and Clinical Immunology: In Practice. 2020 Feb 1;8(2):429-40.
- Johansson SG, Hourihane JB, Bousquet J, Bruijnzeel‐Koomen C, Dreborg S, Haahtela T, Kowalski ML, Mygind N, Ring J, Van Cauwenberge P, van Hage‐Hamsten M. A revised nomenclature for allergy: an EAACI position statement from the EAACI nomenclature task force. Allergy. 2001 Sep;56(9):813-24.
- Romanet‐Manent S, Charpin D, Magnan A, Lanteaume A, Vervloet D, EGEA Cooperative Group. Allergic vs nonallergic asthma: what makes the difference?. Allergy. 2002 Jul;57(7):607-13.
- National Health Service Health A to Z: COPD Overview https://www.nhs.uk/conditions/chronic-obstructive-pulmonary-disease-copd/
- National Health Service Health A to Z: Asthma Treatment https://www.nhs.uk/conditions/asthma/treatment/




