

Do you recognise that unexplained pain on one side of your lower abdomen that doesn't coincide with your menstrual cycle? The one associated with your fertile window that comes back every month?
A benign pre-ovulatory lower abdomen ache that occurs in assigned females at birth (AFAB) mid-cycle (between days 7 and 24) is termed "ovulation pain or Mittelschmerz," as it is more widely known today.
This piece will help you through the complexities of frequent but occasionally puzzling menstrual cycles and understand ovulation pain and its importance in your reproductive process.
Overview
Usually, ovulation discomfort persists until a few years after menarche, when the ovulatory cycles begin. The pain is felt on the same side as the developing follicle, close to the ovaries and ranges in intensity from a dull ache to excruciating agony. The peak of plasma luteinising hormone (LH) levels during the expanding but not ruptured phase of the follicle corresponds with Mittelschmerz. Instead, the prostaglandin-mediated mechanism that LH surge uses to promote ovarian perifollicular smooth muscle contractility may result in pain.1
The following table clarifies the menstrual cycle and aids in understanding ovulation.
| Phases | Mechanism |
| Phase 1 (The follicular or proliferative phase) | The follicular phase's fluctuating length causes the menstrual cycle's variability in the period17-beta-estradiol, or oestrogen, is the primary hormone involved. The activation of the stimulating follicle hormone (FSH) receptors within the follicle at the start of the cycle induces an increase in this hormone. This stage is all about the uterus's endometrial layer growing, increasing the number of stroma and glands with the deepening of the spiral arteries that supply the endometrium with 17-beta-estradiol Through cervix-created channels, 17-beta-estradiol facilitates helpful and friendly sperm entrance with assistance from cervical mucusGraafian follicles develop from primordial follicles at this phase giving rise to mature follicleIt sets for the subsequent process of ovulation |
| Ovulation | Ovulation occurs on day 14 of an average 28-day cycle. High levels of LH help the ovary to release the ovum |
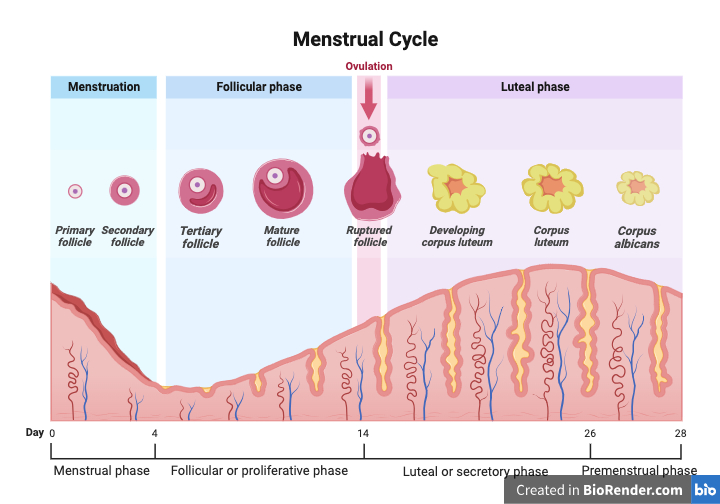
Corpus albicans - Created by: Deepika Rana (Created with BioRender.com)
Understanding ovulation
Around 10 to 12 hours after the LH peak, ovulation happens. Estradiol production by the preovulatory follicle rises sharply, triggering the LH surge. The LH surge starts about 34 to 36 hours before ovulation and can be used to determine the exact time of ovulation. The luteinisation of granulosa cells and the synthesis of progesterone, which is responsible for the mid-cycle FSH surge, are both stimulated by the LH surge. Furthermore, the LH surge triggers the oocyte's reduction division and the resumption of meiosis with the release of the first polar body.2
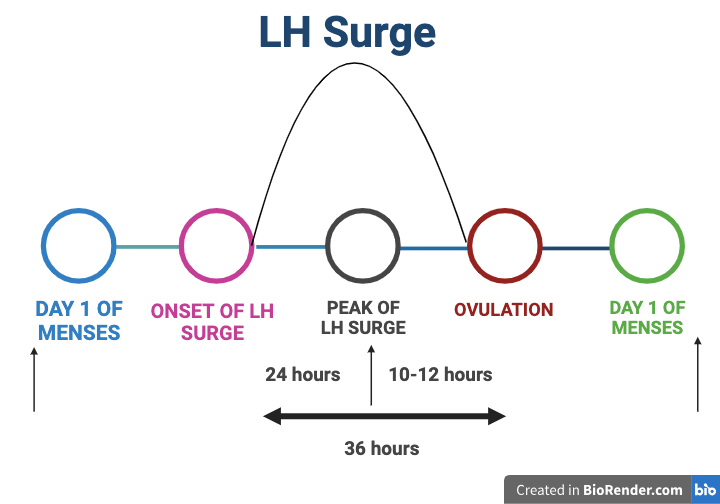
Created by: Deepika Rana (Created with BioRender.com)
In reaction to LH and progesterone, prostaglandins and proteolytic enzymes, including collagenase and plasmin, are elevated.
Prostaglandins trigger the ovary's smooth muscle to contract, which releases the ovum. In humans, ovulation happens randomly from either ovary at any given time throughout a cycle. Some research indicates a greater possibility of pregnancy with right-sided ovulation, which happens more frequently from the right ovary. Prostaglandins E and F series and hydroxyeicosatetraenoic acid (HETE) concentrations in the follicular fluid peak before ovulation.
Prostaglandins can activate proteolytic enzymes, whereas HETEs can trigger hyperemia and angiogenesis. Patients receiving high-dosage prostaglandin synthetase inhibitors, such as Indocin, may have a blockage of prostaglandin synthesis, which successfully prevents follicular rupture. Thus, individuals with infertility refrain from using prostaglandin synthetase inhibitors, particularly during the ovulation period.
Just before the peak of LH, there is a sharp decline in estradiol levels. Progesterone triggers the FSH mid-cycle spike. Elevated FSH levels are assumed to release the oocyte from follicular attachments, activate plasminogen activators, and boost the LH receptors on granulosa cells.
The loss of oestrogen's positive feedback effect, the rise in progesterone's inhibitory feedback effect, or the pituitary's decreased LH content as a result of downregulating gonadotropin hormone-releasing hormone (GnRH) receptors could all be contributing factors to the drop in LH.3
Symptoms of ovulation pain
There are substantial variations in the type and duration of pain related to the Mittelschmerz. Its appearance, time and periodic recurring nature are the characteristics that distinguish it.
- Certain AFAB has a vague ache with the discomfort described as an abrupt squeeze or cramp in either iliac fossa, usually on the side where a growing follicle is situated. The pain goes away in three to twelve hours
- Mild backache in some cases
- A few patients reported feeling sick and having soreness in their pelvis with no pain
- Rectal pain
- Vaginal discharge
- Light vaginal bleeding1,4
Distinguishing ovulation pain from other discomforts
Period and ovulation pain can feel similar but differ concerning time, cause, length, and significance. The illustration shows the variations.
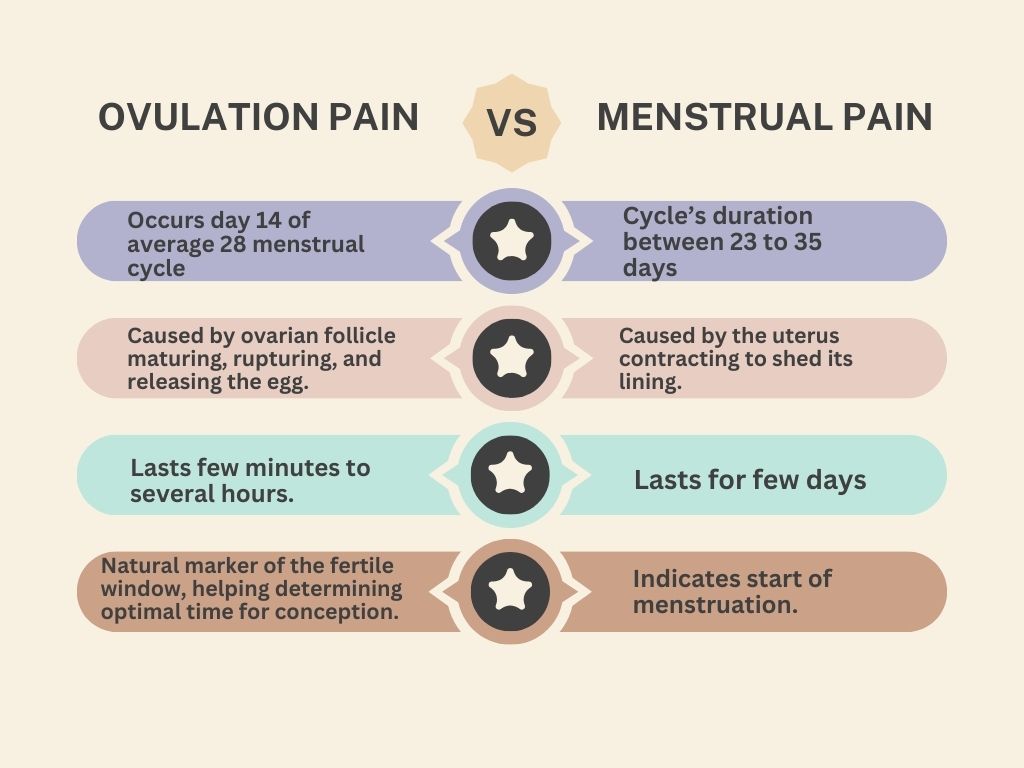
Created by: Deepika Rana (Canva)
The pain associated with ovulation is not a cause for concern. However, if you're in severe pain, consult your healthcare provider. The following list covers the few conditions that call for medical attention.
- Ectopic pregnancy
- Endometriosis
- Pelvic inflammatory disease (PID)
- Ovarian cyst
- Diverticulitis
- Appendicitis
- Inflammatory bowel disease (IBD)
- Bowel obstruction
- Ovarian torsion
- Ovarian hyperstimulation syndrome (OHSS)
- Urinary tract infection (UTI)5
Ovulation pain-relating factors
Hormonal variations
The degree and frequency of ovulation pain can be affected by changes in oestrogen and progesterone levels, particularly the rise in LH that initiates ovulation, as discussed in the previous part of this article.
Lifestyle factors
The habits and way of life that can be changed to significantly impact one's general health and well-being, including fertility, are known as lifestyle factors. Lifestyle factors that can have a positive or negative impact on fertility include drinking, exercise, body weight, diet, smoking habits, using drugs, and consuming alcohol and caffeine.7
Stress
Stress negatively affects AFAB's health by disrupting the hypothalamic-pituitary-gonadal (HPG) axis, leading to ovulatory dysfunction. Hypothalamic hypogonadism can cause such dysfunction to show up as irregular menstruation or infertility. Even though regular menses are a sign of ovulation, they also are related to anovulation. AFAB's health analyses include regular ovulation monitoring—rather than just menstruation—which is essential.8
Reproductive health
Both polycystic ovarian syndrome (PCOS) and endometriosis affect up to 10% of AFAB and harm their quality of life, fertility, and overall health. Though both conditions involve abnormal functioning of the HPG axis and changes to prenatal testosterone levels, PCOS and endometriosis are not yet related.9
Fertility tracking and predicting ovulation pain
Adopting efficient tracking techniques is essential for individuals navigating the waters of fertility and hoping to leverage the insights offered by ovulation pain. The cycle diagram illustrates how different tools interact.
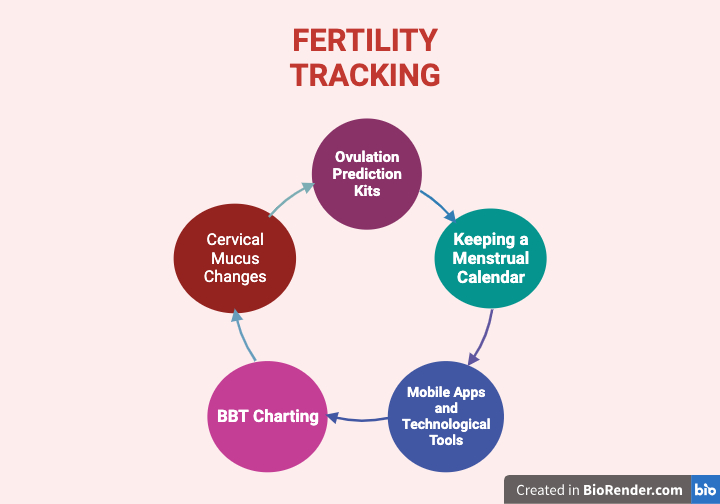
Created by: Deepika Rana (Created with BioRender.com)
Use of ovulation prediction kits
- Ovulation predictor kits (OPKs) are accurate and commercially available and can increase the likelihood of becoming pregnant by timing unprotected sexual activity
- OPKs are an additional tool for managing fertility as they may raise the chance of conception and, in general, have not been shown to increase stress or anxiety, especially in those who do end up pregnant10
Keeping a menstrual calendar
- There are six days in an AFAB's menstrual cycle when sexual activity can lead to pregnancy. This period is called the "fertile window" and includes the five days leading up to ovulation as well as the actual day of ovulation
- The timing of the six fertile days varies from cycle to cycle like the day of ovulation. Before day ten or after day 17 of their menstrual cycle, over 70% of AFAB are in their fertile window11
Mobile apps and technological tools
- Applications can be helpful resources for monitoring and achieving health objectives. Menstrual cycle tracking apps (MCTAs) help users manage their fertility and update on their menstrual cycle and associated signs and symptoms
- MCTAs offer features that broaden users' understanding of the menstrual cycle, and tracking cycles can teach about their bodies' patterns. Apps' algorithmic choices affect their accuracy and biological monitoring as contrasted to calendar techniques and their utility12
BBT measurement
- The thermogenic effect of progesterone causes a rise in basal body temperature (BBT). BBT remains in the lower range during the follicular phase of the menstrual cycle, usually between 97.0°F and 98.0°F, until it reaches its lowest point about one day before ovulation
- Following ovulation, progesterone production in the corpus luteum begins, decreases during the luteal phase and BBT returns to the lower range one to two days before menstruation. Measuring their oral or vaginal temperature every day when they wake up is advised for AFAB interested in figuring out their fertility window
Cervical mucus observation
- Cervical mucus appears differently at various stages during the menstrual cycle. Before ovulation, mucus is thicker and acts as a barrier to sperm
- Cervical mucus will then become thinner and more receptive to sperm penetration during ovulation. At this time, AFAB tends to discharge more water, having the consistency of raw egg white13
Management and relief
As the table below illustrates, navigating ovulation pain requires a combination of mindful management and natural remedies to reduce discomfort resembling period pain.
| Remedy | Explanation |
| Pain relievers | NSAIDs are a group of drugs used to treat pain, like aspirin, naproxen, and ibuprofen. NSAIDs work as analgesics by preventingprostaglandin-synthesising enzyme activity14 |
| Heat therapy | A heating pad applied to the lower abdomen can ease cramps related to painful menstruation and ovulation pain by relaxing the muscles. A warm bath can also have calming relief15 |
| Relaxation | By managing stress and tension, deep breathing exercises, resting, and meditation can help minimise the effects of ovulation pain |
| Hydration | Maintaining adequate hydration can help relieve tense muscles brought on by ovulation discomfort. Consuming 1600–2000 ml of water per day may help reduce the length of menstrual bleeding, the quantity of painkillers taken, and the intensity of pelvic pain16 |
| Exercise | Stretching and yoga are low-intensity exercises that demonstrate the most significant and enduring beneficial effects. It lowers cortisol levels, which may lessen the production of prostaglandins17 |
FAQs
Is there a change in AFAB’s odour during ovulation?
Studies indicate that assigned males at birth (AMAB) might find AFAB's body smell more alluring during the high-fertility ovulatory period than at other times of the menstrual cycle. AMAB's testosterone secretion increased when AFAB's scents radiated from their backs during the ovulatory phase, whereas cortisol secretion decreased when the aromas emitted from their chests during the same period.5
What percentage of AFABs have ovulation pain?
More than 40% of fertile AFAB may get Mittelschmerz, which strikes these individuals nearly every month.1
What are the physiological signs of ovulation?
Urine LH, cervical mucus, and BBT are the physiological signs observed. According to urine LH readings from home monitoring systems, ovulation occurred 91% of the time during the two days of maximum fertility and 97% during the two peak days plus 1. The quality of mucus had a stronger correlation with conception rates. Retrospective in nature, BBT is most effective when used in conjunction with other ovulation indicators.7
Summary
During the menstrual cycle, ovulation pain is a natural and periodic incidence. It's safe to experience ovulation pain. Even though everyone experiences ovulation pain differently, knowing when and how it manifests itself can help people take control of their reproductive health and make wise decisions.
References
- Brott NR, Le JK. Mittelschmerz. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Nov 20]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK549822/
- Thiyagarajan DK, Basit H, Jeanmonod R. Physiology, menstrual cycle. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2023 Nov 20]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK500020/
- Reed BG, Carr BR. The normal menstrual cycle and the control of ovulation. In: Feingold KR, Anawalt B, Blackman MR, Boyce A, Chrousos G, Corpas E, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000 [cited 2023 Nov 20]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK279054/
- Wehrs RE. The Mittelschmerz [Internet]. DigitalCommons@UNMC. University of Nebraska Medical Center; 1952 [cited 2023 Nov 21]. Available from: https://digitalcommons.unmc.edu/cgi/viewcontent.cgi?article=2869&context=mdtheses
- Tarumi W, Shinohara K. Women’s body odour during the ovulatory phase modulates testosterone and cortisol levels in men. PLoS One [Internet]. 2020 Mar 31 [cited 2023 Nov 21];15(3):e0230838. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7108710/
- Gynecologic pain: practice essentials, acute pelvic pain, recurrent pelvic pain. 2023 Jun 13 [cited 2023 Nov 21]; Available from: https://emedicine.medscape.com/article/270450-overview
- Owen M. Physiological signs of ovulation and fertility are readily observable by women. The Linacre Quarterly [Internet]. 2013 Feb [cited 2023 Nov 21];80(1):17. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6081768/
- Sharma R, Biedenharn KR, Fedor JM, Agarwal A. Lifestyle factors and reproductive health: taking control of your fertility. Reproductive Biology and Endocrinology : RB&E [Internet]. 2013 [cited 2023 Nov 22];11:66. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3717046/
- Vigil P, Meléndez J, Soto H, Petkovic G, Bernal YA, Molina S. Chronic stress and ovulatory dysfunction: implications in times of COVID-19. Front Glob Womens Health [Internet]. 2022 May 23 [cited 2023 Nov 22];3:866104. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9168655/
- Dinsdale NL, Crespi BJ. Endometriosis and polycystic ovary syndrome are diametric disorders. Evol Appl [Internet]. 2021 May 14 [cited 2023 Nov 22];14(7):1693–715. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8288001/
- Yeh PT, Kennedy CE, Van der Poel S, Matsaseng T, Bernard L, Narasimhan M. Should home-based ovulation predictor kits be offered as an additional approach for fertility management for women and couples desiring pregnancy? A systematic review and meta-analysis. BMJ Glob Health [Internet]. 2019 Apr 25 [cited 2023 Nov 22];4(2):e001403. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6509595/
- Wilcox AJ, Dunson D, Baird DD. The timing of the “fertile window” in the menstrual cycle: day specific estimates from a prospective study. BMJ [Internet]. 2000 Nov 18 [cited 2023 Nov 22];321(7271):1259–62. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC27529/
- Schantz JS, Fernandez CSP, Anne Marie ZJ. Menstrual cycle tracking applications and the potential for epidemiological research: a comprehensive review of the literature. Curr Epidemiol Rep [Internet]. 2021 Mar [cited 2023 Nov 22];8(1):9–19. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8162175/
- Su H, Yi Y, Wei T, Chang T, Cheng C. Detection of ovulation, a review of currently available methods. Bioeng Transl Med [Internet]. 2017 May 16 [cited 2023 Nov 22];2(3):238–46. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5689497/
- JUKIC AMZ, PADIYARA P, BRACKEN MB, MCCONNAUGHEY DR, STEINER AZ. Analgesic use at ovulation and implantation and human fertility. Am J Obstet Gynecol [Internet]. 2020 May [cited 2023 Nov 22];222(5):476.e1-476.e11. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7195999/
- Jo J, Lee SH. Heat therapy for primary dysmenorrhea: A systematic review and meta-analysis of its effects on pain relief and quality of life. Sci Rep [Internet]. 2018 Nov 2 [cited 2023 Nov 22];8:16252. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6214933/
- Torkan B, Mousavi M, Dehghani S, Hajipour L, Sadeghi N, Ziaei Rad M, et al. The role of water intake in the severity of pain and menstrual distress among females suffering from primary dysmenorrhea: a semi-experimental study. BMC Women’s Health [Internet]. 2021 Jan 28 [cited 2023 Nov 23];21(1):40. Available from: https://doi.org/10.1186/s12905-021-01184-w




